
I contributed to an article intended for maurice.nl (title: "Title: How safe and effective are the vaccines?".) Unexplained excess mortality, which virus varia has been calling attention to since August 2021, plays an important role in the article. That's why it shouldn't be missing from this site, including some last minute additions in purple.
EDIT: We present here a calculation with limit values in which vaccine effectiveness is set at a maximum of 100% and where excess mortality for the maximum 100% is also caused by vaccinations. Both values are hypothetical. In reality, vaccinations may only contribute 25%, 5% or 0.5% to excess mortality, and the effectiveness is, for example, 50%. In a next blog we will calculate other values. Given the possible scenarios, it is difficult to understand that the exclusion of the vaccines as a (partial) cause of the excess mortality is not given the highest priority, by means of independent research on public data.
How safe and effective are the vaccines?
By Herman Steigstra, Jillis Kriek, Lilian Namink and Anton Theunissen
Autumn campaign OMT-V
Preparations are already being made to start vaccinating in the autumn: New corona vaccination in autumn for everyone from the age of 12. Although the cautious urge now seems to be subsiding, it still worries us that the vaccines are being touted as "Safe and effective”. However, there are now also signals at the central government that the effect of vaccination may be only 4 weeks protection against infection. This is a statement that can be read there:
We now know that you can still get corona even with a vaccination. The vaccine protects against infection for about 4 weeks. So you can still get sick even with a repeat vaccination. However, the vaccine does prevent you from becoming seriously ill. You can also see this in the admission figures from hospitals. In people over 60, a decrease in protection can be seen 3 months after the last vaccination. That is why the repeat vaccination is so important for this group of people in particular.
There is still a lack of proactive information and good figures. A lot has already been published about the effectiveness of the vaccines and it now seems that the outcome of each study is mainly determined by the preconditions. For example, you are counted as unvaccinated if you die within two weeks of vaccination. This results in a strongly distorted VE.
Information government
The government should be obliged to provide clear information and also be actively obliged to follow up with a form after vaccinations. After all, you are not going to get a vaccination for Yellow Fever in the Netherlands if you do not go to a tropical area where Yellow Fever is prevalent. You weigh your risks and then, in consultation with the doctor, you make a decision.
The government should also be obliged to actively inform the public of the possibility of reporting the side effects to the Lareb.
This is how it should be when taking a vaccine against SARS-CoV-2, but the government only states that it "Safe and effective" is. Meanwhile, there are more and more voices that question both aspects. So what you would like now is to be able to weigh up the effectiveness that is still there and the risks that vaccination entails. Unfortunately, there are only indications for both aspects and the government is still not expressing any reservations. Apparently the government is only concerned with maintaining the existing narrative and we only have suspicions about the underlying agenda. The fact that the 17 million autumn boosters have already been ordered will certainly play a role in the considerations.
Our information
Through this article we want to try to provide a bit of information, based on a number of assumptions, all of which are uncertain. This information should therefore be seen as a framework that can be helpful to get an impression of what everyone's opportunities are. Then you could start tinkering with each of the assumptions, turn the knobs and see what happens.
What information do we have and how sure are we of it:
- The arrival of a new variant. It will probably come and how contagious will it be? We assume here that a new variant will be able to cause an equal number of deaths, but the trend seems to be decreasing with the arrival of new variants.
- Will the new vaccine be effective for the new variant that we do not yet know? In the examples, we will assume that the new vaccine is 100% effective against a new variant and will also have an unlimited duration of protection. It is unlikely that this will be the case, but it will allow us to explore the limits of the possibilities. A VE that is between 0% and 50% seems more realistic and a protection duration of 1-3 months also seems more likely.
- What about excess mortality? We can see from the CBS figures that there is a very significant excess mortality. It is not certain that it was caused by vaccination, but it is likely and in this article we assume that it is. As long as the cause of this excess mortality has not been proven, we must take this seriously into account.
The basic figures
We therefore assume that vaccination will soon not only be 100% effective, but also fully responsible for the observed excess mortality in the past year.
We only use the mortality figures for the Omicron (Covid-21) epidemic from 1 January 2022 to the end of July. Reliable figures are still a problem. The RIVM seems to come up with slightly too low death figures, while the weekly figures from Statistics Netherlands are now more than three times as high as those from the RIVM.

If we compare the excess mortality figures with the figures from the RIVM, we have more confidence in the RIVM than the CBS.
We also see in the figures from Statistics Netherlands that the number of deaths from other respiratory diseases went down by 60% in the winter of 2020/21. This gives the impression that corona has supplanted other lung diseases.

More realistic is the assumption that the death reports mention several causes and if corona is one of them, it is often used as the primary cause of death. It would be a plausible explanation that the CBS figures for corona are much higher than those of the RIVM. It cries out for further explanation!
We will therefore limit ourselves here to the official RIVM figures, also because the CBS figures for the second quarter of 2022 will not be available for another three months.
The excess mortality figures are derived from the CBS website. The problem, however, is that the age cohorts there are different from the age cohorts used by the RIVM. We had to correct for that.
We calculated the excess mortality over the period from May 2021 to July 2022. If we assume that excess mortality is the result of vaccination, then we should start counting there. But it is an assumption that a new round of vaccination will cause proportionally the same excess mortality.
Not only in the Netherlands...
In addition to our own figures, figures have also been published by the government in Germany on damage caused by vaccination. These articles were published recently:
- Half a million medical treatments by vaccines at one German health insurance fund.
- German hospital federation demands withdrawal of vaccination obligation for healthcare staff.
- Serious side effects exceed the risk of hospitalization with COVID-19 in the Swedish population.
- 0,2 Suspicioussmeldungen pro 1.000 Impfdosen beträgt die Melderate ans @PEI_Germany für schwerwiegende Reaktionen.
According to reports in Germany, 1 in 5000 vaccinations (so in about 1 in 1250 vaccinated people) results in very serious side effects, which are actually reported. In the Netherlands, we see that there is an excess mortality of 11,623, while there are around 11 million vaccinated people. So if excess mortality is caused by vaccination (still an assumption) then about 1 in 1000 vaccinated people die. So that figure corresponds surprisingly well with the German findings.
It is remarkable that LAREB does not think it sees these figures. According to estimates, the figures of LAREB 15 times lower than suspected.
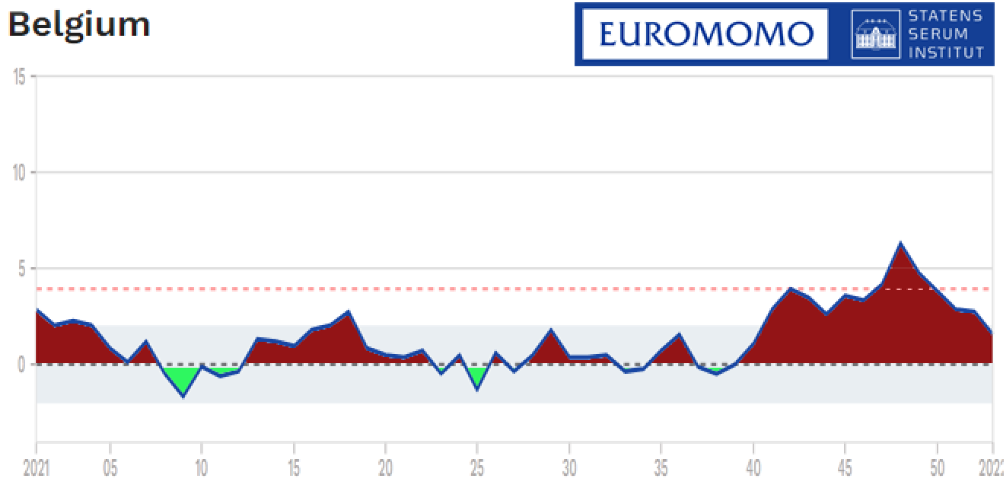
Virusvaria bonus: Belgium, Spain, Canada...


Vaccine Effectiveness (VE)
Many studies have already been published on this subject and we are not going to deal with them in this article. We are only providing a framework here and assume for the sake of convenience that the vaccines being developed for the as yet unknown variant that could appear in the autumn can provide full protection for it. We also assume that the autumn variant would cause as many deaths as all Omicron variants combined. So from a prevention point of view, the most powerful use of the vaccines we can imagine.
| Deaths/100,000 | ||
| Age | Omikron variants | Influenza (indicative) |
| 0-50 years | 0,13 | 0,33 |
| 50-59 years | 1,4 | 4,2 |
| 60-69 years | 5,4 | 12,4 |
| 70-79 years | 23 | 29 |
| 80+ | 113 | 131 |
Because the figures broken down by age are only available until the beginning of February 2022, the figures were used from the beginning of the epidemic and then converted on the basis of the total number of Omicron deaths since 1 January 2022 (during the entire epidemic, 22,469 people died of corona until the end of July 2022, of which 1,554 died of the Omicron variant).
Net excess mortality
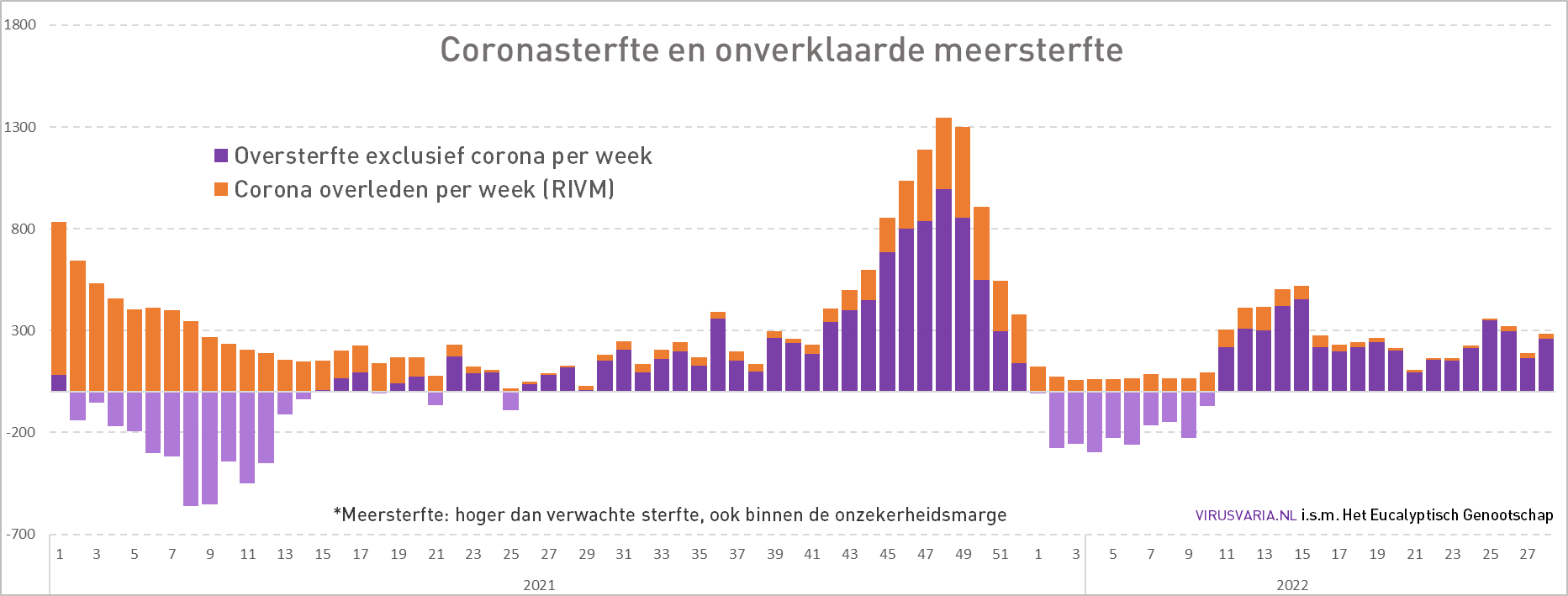
If we want to know what the possible consequence of the vaccination is that we see in the excess mortality figures, we have to calculate the net effect. That is the excess mortality as reported by CBS on its website, after deducting the number of deaths from corona itself, and we therefore use the RIVM figures for this. This creates this graph for "Net excess mortality":

We see in this graph that during the first year of the epidemic, net excess mortality is virtually nil. Only an undermortality in the first two months, because no people died of influenza at that time, a normal phenomenon.
From January 2021 to May 2021, the Alpha variant raged here and caused around 6000 deaths. On the other hand, there was a sharp reduction in mortality from other causes, resulting in a total net undermortality of almost 4000. We see this in the graph as the descending red line until July.
From July 2021 onwards, we will then see the trend in excess mortality emerging. An average of 15 unexplained deaths per day for the 80+ age group and 13 per day for the 65-80 year olds. For 0-65 years, the net excess mortality is around 1 per day.
If we convert these figures into the number of deaths per 100,000 inhabitants, these are the probabilities per age group:
| Hypothesis: 100% excess mortality attributed to vaccines with 100% effectiveness | ||
| Age | Excess mortality/100,000 | Chance of death |
| 0-50 years | 3,1 | 24 X |
| 50-59 years | 58 | 42 X |
| 60-69 years | 113 | 21 X |
| 70-79 years | 221 | 10 X |
| 80+ | 687 | 6 X |
Because CBS does not provide a breakdown for the ages under 65, we have manually split these groups based on an estimate. The right column shows the risk of dying from the vaccination compared to the risk of dying from corona. So we see that for all ages, vaccination increases the risk of dying by at least a factor of 6 for the 80+ group to as much as 42 times for the ages 50-59 years.
What is now becoming visible, but which we are not yet taking into account, is a possible doubling of this excess mortality that we seem to have seen for four weeks. Whether that is the result of the second booster round In April (in week 14 50% vaccination coverage for the elderly) is of course still unclear. In our calculations, we still assume 15/day, 13/day and 1/day.
The end result of this scenario
As mentioned, we assume a 100% protection of the vaccine and caused excess mortality equal to the observed excess mortality as a result of the previous vaccination rounds. We can then compare the expected number of deaths per 100,000 inhabitants in a graph for each age group:

The blue bars therefore indicate the number of deaths per 100,000 that will be prevented by vaccination for each age group. We assume that everyone is vaccinated and also a VE of 100%. The red bars are the expected excess mortality as a result of vaccination.
We see here that depending on the age group, vaccination has increased the risk of dying between 6 and 42 times.
IC occupancy
In addition to the personal risk for those who have or have not been vaccinated, there is also the government's concern for overburdening the healthcare system and in particular the ICU capacity. We have also visualized these figures and we see this graph with the cumulative number of days in the ICU for corona patients:

The first thing that strikes you is that the trend in the number of occupied beds is almost straight from autumn 2020 to the dawn of spring 2021. Vaccination started in the winter of 2020/21 and it does not seem to have had any impact on ICU occupancy. In fact, the number of hospital days counted from the start of vaccination (147,786) is greater than the number of hospital days before vaccination started (131,229). From the arrival of the Omicron variant, ICU occupancy dropped rapidly. At the peak of the epidemic on April 7, 2020, there were 1424 in the ICUs and now that number is around 40, while we are now at the peak of the "Summer Wave". Even with an "Autumn wave", an overcrowding of ICUs with this mild Omicron variant is no longer to be expected.
The OMT-V advice
On 26 July, the new Outbreak Management Team Vaccination (OMT-V) issued an advice on a new round of vaccinations in the second half of September: Opinion 1st OMT-V on COVID-19. The first thing that strikes us is that no figure is mentioned (neither in the opinion nor in the annex), only assumptions and the recommendation to offer the vaccine from the age of 12. Especially for healthcare personnel, because they are also seen as possible spreaders of the virus. Furthermore, only ifs and buts without numerical substantiation. It may be possible to add the figures presented in this article as an addendum to the advice.
Conclusions
Based on an assumed VE of 100% and a risk of death based on the CBS excess mortality figures over the past year, it must be concluded that in a general sense vaccination only increases the risk. It should be noted, however, that the figures obtained from the past do not give any guarantee for the future. The assumed effectiveness of the vaccines yet to be marketed for the as yet unknown variant in September will probably also be well below 100%. The degree of side effects is of course still unknown. The government's statement that the vaccine "Safe and effective" is under heavy pressure.
Based on the above considerations, the risk of dying from vaccination is estimated to be at least a factor of 6 higher than reducing the risk of dying from corona. If the vaccines offer a protection lower than 100%, the risk even increases proportionally. On the other hand, if the side effects of the new vaccines are less than we fear based on the experience with the current vaccines, then the risk will also be proportionately smaller. But we can only determine that risk in a year's time. It justifies a clear warning and "informed consent" when giving the vaccine.
Vaccination must remain a personal consideration. If someone is convinced that they will benefit from vaccination, it should remain possible to get the shot. Even if it would only be to achieve a certain peace of mind. But vaccination under the age of 60 never seems to have any advantage.
Looking back at the waves since vaccination until the end of 2021, vaccination seems to have caused more damage than protection. There were about 7,000 deaths from corona compared to an excess mortality of 16,000 that is still rising. We also see a strong decrease in deaths from "other diseases", which suggests that a significant proportion is "with corona". It seems difficult to maintain that the vaccines "Safe and effective".
P.S. (in your own name!): In any case, try to prevent people from vaccinating their children unless there is a very good reason for it. I see that as everyone's responsibility.
Hi Anton, your last sentence: 'Try to prevent...' DO NOT' remove it, because now you say that parents should get vaccinated...
Tjee yes – such a typical quick final correction by mobile because I didn't read my own sentence properly! Thank you Frans!
I would also put 'in any case' before 'preventable' – reads a bit easier.
Good article. I would replace malaria shot with another one. There is no such thing as a malaria shot.
Thank you very much for all your efforts and clear publications!
Replaced by "Yellow Fever". Thanks!
" Try to prevent people from at least not vaccinating their children ".
and none of the FOUR authors have noticed that this is the reverse of what they want to say?
The other authors have not seen this. It also says "in my own name" so it is entirely my own fault and it is in purple, which has been explained to be additions to the original article. Has since been corrected, thanks for the attention!
What I do find very special (but maybe I'm drawing the wrong conclusion):
The fact that you did not observe any excess mortality during the famous first wave (March/April 2020).
On the other hand, not very strange, because it was mainly people over 80 and people with underlying suffering who were affected. Who would probably have died of a flu or another condition in a different situation. But they do count in the Covid narrative. During that period, mortality from other causes is miraculously a lot lower than normal. This in stark contrast to the later periods (after vaccination). You mainly focus on the period after the vaccinations have started. But the excess mortality in March/April 2020 (lack thereof) also seems very interesting to me.
The RIVM site shows a shockingly high number of Covid deaths. More than 22,000! This is very misleading, because cumulatively over at least 3 flu seasons. Moreover, I don't believe it. As you have already observed, there are often several causes of death, we are talking about WITH Covid. Normally, you count the number of deaths per year for a specific cause of death. The absolute number of >22,000 is scare tactics and comparing apples with oranges.
Good piece again. I was already out, by the way:-). Never got a shot and it will stay that way.
This piece zooms in on the vaccination period. You might like these: https://virusvaria.nl/covid-19-is-niet-doodsoorzaak-nr-1/
(wrong avatar after moving under the correct comment)
This is exactly what I meant, Anton. Maybe I had even read it already. I don't remember, but it fills in exactly the doubts I had about that period. I had already seen that a number of causes of death were miraculously lower, but you have figured it all out.
It remains relevant, because by presenting this period in a certain way, the government has frightened most of the population.
So, just shared this well-researched, honest story on Facebook. Not that I have any friends anymore, they unfriended me a long time ago after previous sharing actions of Virusvaria.
I'm sorry to hear that Lars. Some pieces may be a bit too activist, but there are also sensible pieces among them. If they drop out, well... Good that you keep your back straight!
It is certainly a good article, but I would really like to draw the readers' attention to the package leaflets of the vaccines.
You can only find them indirectly on central government. For Astra Cenica, you go to the information via a button leaflets for caregivers or something like that. You have to click through somewhere to see what's in it.
The first is a component that comes from chimpanzees.
I don't know anything about medicines, but it is good to know that it contains animal preparations.
I am thinking of the transmission of monkeypox. Why doesn't the government report on this?
And why do you immediately see the entire package leaflet? And what are the conditions that are attached to the approval?
These are all risk factors, which you must be able to weigh up in complete freedom. So that's why I think this info should be included and therefore says nothing about how wise or unwise it is to take a vaccine or not.
If the government insists again, I want to enforce complete and easily accessible information