
Since it is perfectly understandable that perusing a 168-page numerical report is shelved by this and that, I thought it would be an idea to pick some elements from it. This will give an impression of what is covered and demonstrated. I will try to describe the results of an entire chapter in a few paragraphs, so no underpinning or references. Chapter 6 is treated in more detail because new data were used in that chapter, providing real new insights. At other points, it deepens phenomena we already suspected.
Short link to this article: https://t.ly/SdCRs
Chapter 1: Introduction and justification
The authors point to the complexity of the issue and the imperfections of the available data, which are discussed in detail in the report. In doing so, they realise that this is a politically explosive issue. They consider the accessibility of the data insufficient.
Chapter 2: Excess mortality patterns
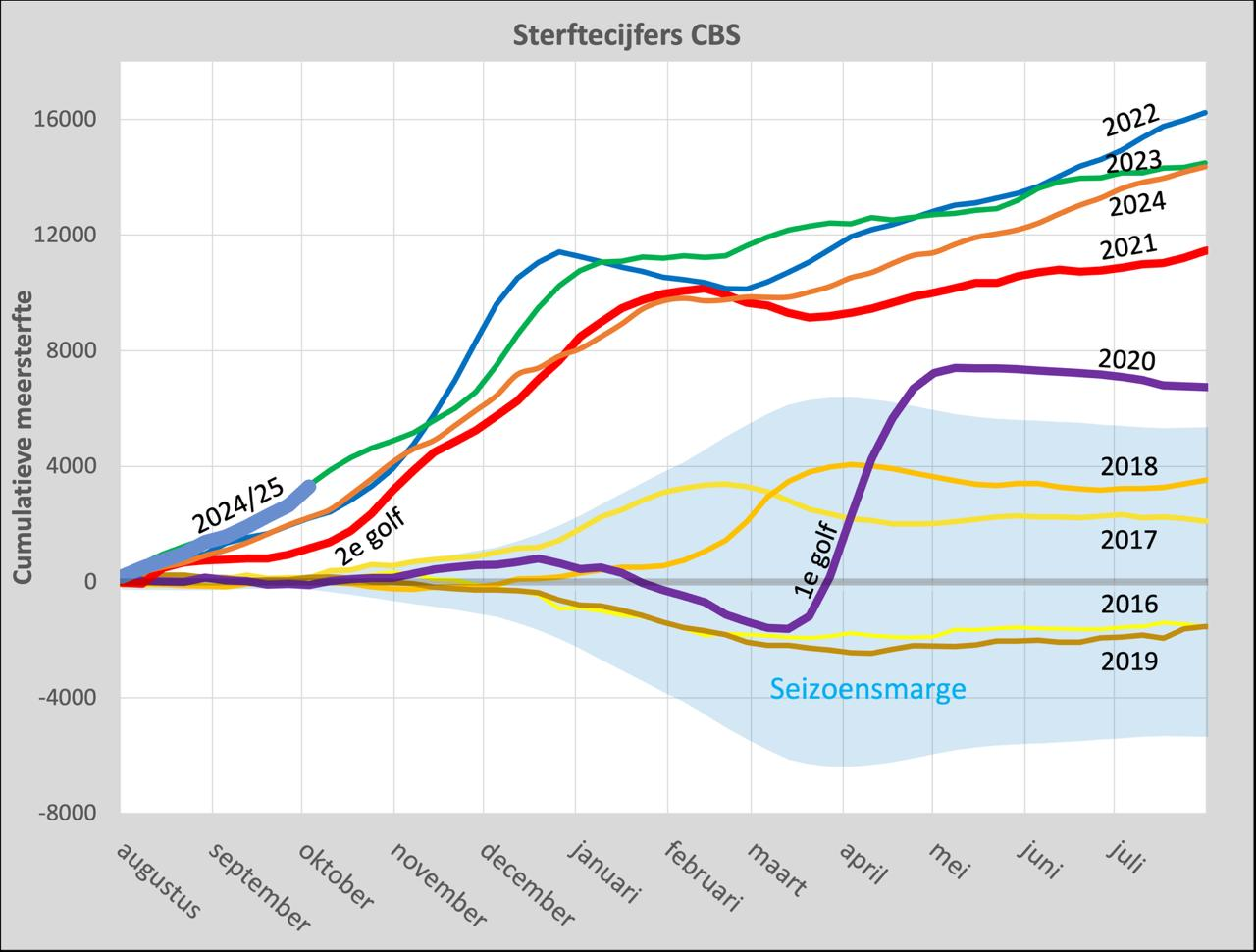
There is no doubt that, since mid-2021, there has been a substantial unaccounted-for excess mortality that continues to this day.
The weekly bandwidth is considered a ‘safe’ limit by government agencies and hence in the media. When assessing longer periods, this is misleading. Variations per week are percentage-wise much larger than per month, quarter or year. The bandwidth narrows considerably at longer periods.
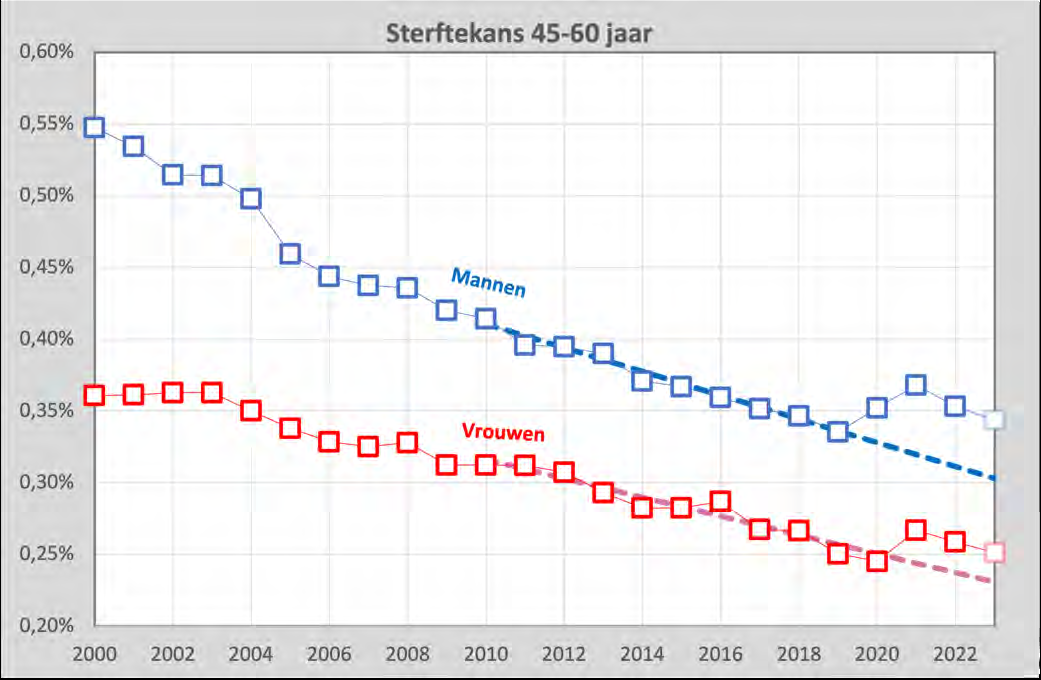
At higher mortality projections, excess mortality decreases. The government institutes include the misunderstood excess mortality years in their calculations. Consequently, the predicted mortality becomes higher, resulting in a reduction in excess mortality. Therefore, this study uses recalculated mortality projections based on mortality probabilities by age and size of age groups based on 2010-2019 statistics.
This allows for fine-grained analyses. See here in a graph the mortality probabilities for men and women aged 45-60 years, from 2010-2023.
What is not included in the graph above is the expected under-mortality after excess mortality. This is taken into account in the study. Missed under-mortality contributes to excess mortality. This additional excess mortality is not included in government communication.
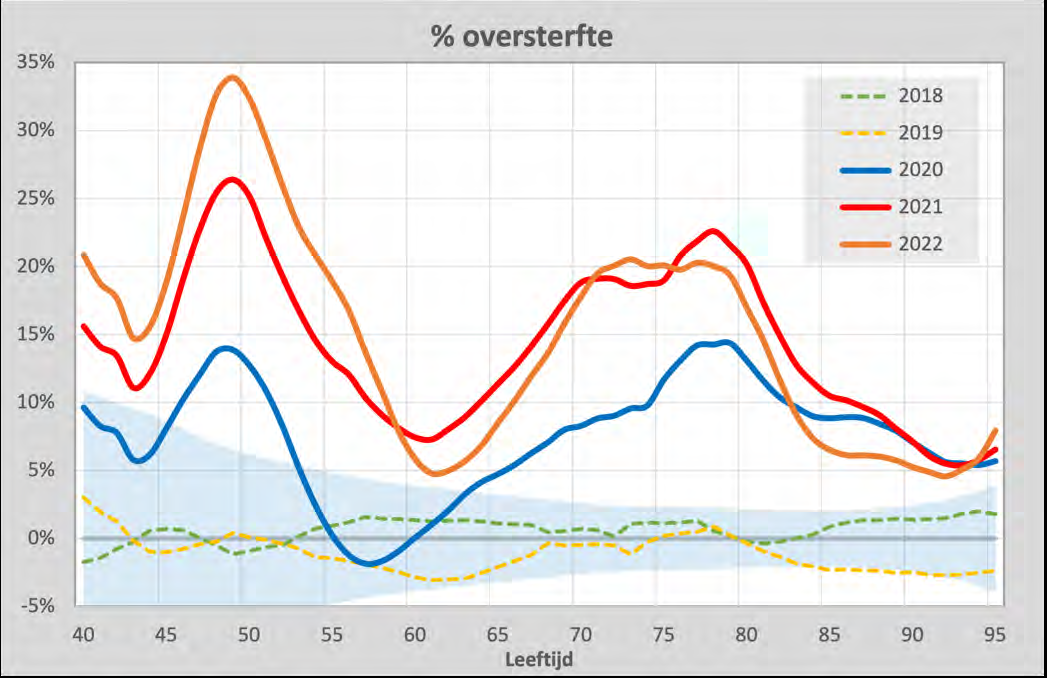
Excess mortality rates vary by age group. After 'full' Corona year 2020, in 2021 and 2022 they are at roughly around 10% to 15%.
Also, by 2021, the average age of death drops by 5 years. So people are dying younger. This continues in 2022, when corona no longer plays a significant role. The duration and quantity of this phenomenon exclude that the main cause is to be found in delayed care or in (undiagnosed) Covid-19.
Chapter 3: Adverse reactions in a trial and in a report database
Examples that cause concern.
Safe? AstraZeneca: a double-blind trial shows that the jab caused serious side effects. This does not fit the predicate 'safe', on which public health policy is based. There is every reason to be concerned about at least this particular vaccine on the basis of these data.
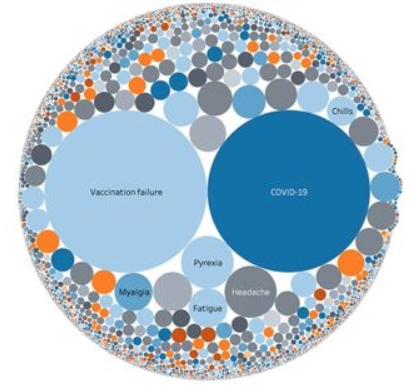
Effective? EMA (European Medicine Agency): One of the two most common reports after Covid-19 vaccination is "Covid-19", at least two weeks after vaccination. If the infection occurs in the first two weeks, the notification is not classified as "Covid-19" but as "Vaccination Failure". Those two reports added together means that getting the disease is by far the most common side effect of the intended protector against that very disease. This calls into question its effectiveness.
Chapter 4: meta-analysis of peer-reviewed literature
international differences in periods of virus spread, vaccination campaigns and seasonal influences make the juxtaposition of studies challenging. Systematically designed studies could facilitate this. Unfortunately, the diversity in topics, methodology, definitions (even terms such as ‘vaccination status’ and ‘vaccine effectiveness’ are defined differently) and the varying quality of the studies make it impossible to find a broad basis for general statements. Some conclusions that can be drawn are:
- Considering the variety of findings, there could be no question of "Follow the Science".
- There is publication bias. Vaccine criticism is not readily embraced in the healthcare sector. Again, polarisation distorts information exchange.
- A striking number of studies show that not too much should be expected from peer review. Illustratively, even studies with unclear definitions of crucial concepts have been accepted for publication despite (or thanks to) a review process, while repeatedly showing missing raw data, debatable measurement periods, black box modelling, discrepancies between reporting and data.
- Wherever there is evidence of high vaccine efficacy, the Healthy Vaccinee Effect is ignored. A separate chapter is devoted to this.
Chapter 5: Macro Analysis
A CBS publication dd 23 November 2023 allows for analyses of protection against Covid-19 mortality. These show that people who got only one shot died from Covid more often than others in the first 4 weeks after the shot: a negative VE, even without observing the HVE. (HVE: People who forgo vaccination often have health reasons for doing so. This distorts mortality rates in favour of vaccination).
Other CBS publications also show correlations between vaccination volume and mortality. The Ministry of Health, which does confirm the correlations, argues that these correlations do not imply causality and therefore sees no need for investigation.
Zooming out, it is striking that the mortality pattern is changing: the deviant behaviour of the second wave compared to the first starts with the vaccination campaign in 2021. The picture fits a scenario in which vaccination generates short-term damage, in the form of mortality. The further course may indicate a reduced general resistance to seasonal viruses. More on this in Chapter 8.
Chapter 6: CBS microdata
[Note: the following is just a selection from the 60-plus page chapter by Bram Bakker. It doesn't do justice to the quality of the work. The real value of this study lies in the verifiable substantiation, insofar as CBS allows. Many questions remain unanswered, mainly due to data gaps. This makes the call for (re)construction of reliable data even louder.
The analyses were done in the CBS microdata environment, with data at the individual person level, including the CIMS vaccination database used for the ZonMw Excess Mortality programme line. A large part of this chapter describes the methods and techniques used to look at the data. The attempts to distill meaningful data from it from different statistical angles are impressive and are described in detail. Below is only a selection of the results. Note that these statements are thus hard-wired from the source data, not hypotheses based on public reports.
A more comprehensive, substantive summary was made by Jan Bonte on x. Also read the furious column of Maurice de Hond. Herman Steigstra posted an in-depth article on LinkedIn].
Slightly increased mortality is visible during both the basic vaccination rounds and the booster round, especially in older age groups. This can be seen in particular in the unvaccinated groups and to a lesser extent in vaccinated groups. Covid mortality is also slightly increased, but represents only a small part of the excess mortality and cannot serve as an explanation.
The Healthy Vaccinee Effect is a well-known phenomenon. Vaccinated people are generally much healthier than unvaccinated people, including people for whom vaccination no longer makes sense. These will die as unvaccinated and count heavily in the statistics; After all, there are relatively many, compared to the small minority of unvaccinated people. Since this has not been corrected for, a high VE (vaccine effectiveness) is the result. Indeed, as a result, the unvaccinated are doing much worse than the vaccinated. This HVE effect, and thus the measured vaccine effectiveness, normally decreases again after these vulnerable unvaccinated people have died, and that is what we see in the figures.
If this effect is taken into account, there is no actual vaccine protection left. In the younger groups, mortality from Covid-19 is negligible anyway.
Another point: there is a group of vaccinated people (about 7%) who did not consent to further research with their data. Those from this group who died were counted at ‘unvaccinated’. In addition, deceased people were not recorded as ‘vaccinated’ who had been immunised. When the register was updated after they died, with delays of a week or more occurring, they were no longer registered living persons. At least that is one of the possible explanations given in the report.
Note: after the publication of the report, this statement was firmly substantiated on X by @leon1969. Click here to read more (This was not part of the report)
He concludes:
- people who died between the start of the vaccination campaign (and at least 9 December 2021) immediately after being vaccinated for the first, or second/third time, ended up (in part, depending on the delivery of the vaccination timing) as unvaccinated deaths in the reports.
- a huge number of people exchanged the temporary for the eternal because of vaccinations. The risk of death increased with each vaccination.
He explains the implications for public health policy in This follow-up tweet.
Due to these gaps (HVE, 7%, registration process), both the reported VE and the safety of the vaccines have been presented much more favorably than they actually are.
For myocarditis, both SARS-CoV2 and vaccinations appear to affect the number of myocarditis diagnoses, with the combination being more detrimental.
In various ways, the data are shown to lead to such absurd conclusions that there must be massive data contamination. Concrete example from the report: vaccinated seventy-somethings would be 98.4% less likely to die in the first 4 weeks than unvaccinated ones, regardless of cause of death (p91). HVE cannot correct away this protection from any death. Thus, the quality of the data is questionable.
The reported very high Vaccine Effectiveness, both in terms of Relative and Absolute Risk Reduction, and both for Covid and for non-Covid/ACM, is actually based on the unrealistically increased mortality of unvaccinated people, compared to the normal mortality pattern for people of that age.
In absolute terms, the 'protection' provided by the corona vaccines against mortality from Covid is much lower than the concomitant 'protection' against mortality from something else. Again, this is clearly a signal that indicates impure data.
The subsequent section, with mortality analyses by 4-week period, broadly confirms the results of the previous analyses. The tone becomes slightly more firm. The HVE does not fit the increased overall mortality during the peaks of the vaccination campaigns because a pure HVE effect changes just the distribution of deaths, not the total number of deaths. All the figures suggest that for all younger groups, vaccinations were at best ineffective and therefore pointless.
The first booster, which is being looked at separately, is also due to the presumed VE to the extremely increased mortality among the "unvaccinated". The increased overall mortality again indicates that it is not only the HVE that plays a role here. Covid-19 has a small share in the total increase in mortality.
CBS/RIVM does not notice the artefacts or simply ignores or downplays them.
For younger groups (from year of birth 1960 or thereabouts) the VE is most likely negligible or perhaps even net negative. No one can really make a statement about long-term damage due to a lack of reliable data.
The small increases in overall mortality of different birth year groups move synchronously with the respective vaccination rounds.
A separate and extensive chapter is devoted to heart failure (myocarditis, etc.). The clearest safety signal is found in the youngest group, 1980-2020, with a greatly increased risk of the condition around the primary vaccination (dose 1) and also in the second half of 2021.
Chapter 7: Reliability of the data
Underlying this chapter is the work of Wouter Aukema, who, among other things, has provided insight into the EMA data. Again, problems with the CIMS register are cited. Graphs show how records have been deleted. The reasons for this have never been explained. The ECDC and Minister Kuipers confirmed that records of deceased (and emigrated) persons are not included. The correction that was promised on this never took place.
Neither is it clear what happened to the ‘failed vaccinations’ mentioned in Chapter 3.
Following a FOI request, RIVM provided the data (records) of all people who were both vaccinated and died between January 2021 and January 2024. However, vaccinations after April 2022 are missing, even though vaccinations were carried out. The part that does seem to be complete shows, for example, that people over 80 had a mortality risk of 0.0037 within one week after the first vaccination. It normally fluctuates around 0.002 per week. The risk of mortality was therefore almost twice as high for them in the first week after vaccination.
[Note: combining this data with the non-registration of people who died shortly after vaccination is in line with the previously observed increase in the VE.]
Chapter 8: Medical Considerations
[Note: now I have to be careful because Jan Bonte co-authored this]
This chapter was produced with the cooperation of Jan Bonte and Jona Walk.
These medics have also seen that there has been excess mortality since the introduction of these vaccines in the Netherlands and this leads them to wonder whether there can be a medical relationship between these two phenomena. An earlier meta-analysis showed that the mRNA vaccines do not reduce overall mortality in any case, which is an important test. No statement could yet be made about medium- and long-term effects.
They discuss the possible mechanisms of these vaccines, which can cause side effects. How often they actually occur is the domain of statisticians.
Studies at the population level indicate that there is an increased risk of myocarditis/pericarditis (inflammation of the heart muscle and inflammation of the pericardium), especially in boys and men aged 12 to 30 years, menstrual disorders and vascular occlusions in the retina of the eye, resulting in partial or total blindness.
Cases have been described in which mRNA derived from the vaccine was found: severe and fatal inflammation of the brain, a severe polymyositis (generalized muscle inflammation), a case involving severe inflammation of the liver, a case of a severe recurrence of a herpes zoster (shingles), thyroid abnormalities, kidney disease, and a range of skin abnormalities.
Not all of these symptoms result in mortality, just like the very common fever, muscle aches, chills, fatigue and headache. For people with a relatively high probability of dying in the coming weeks or months, this impact of the vaccination may bring forward the moment of death. This is followed by a list of cases of healthy people with fatal inflammatory reactions and heart failure, all with serious suspicion of vaccination.
Autoimmune diseases can be triggered by Covid-19 and/or vaccination. Most of the time, these diseases do not lead to immediate death, but increase the risk of premature death in the medium and especially long term.
Here, too, special attention is paid to myocarditis in young people, also repeatedly demonstrated with pathological examinations. The big question for the medical profession is always the incidence: how often does it occur? Lareb's statement that Covid-19 leads to myocarditis more often than vaccination is not supported by the available data. The study design of the study cited by Lareb is inadequate for several reasons. For example, the incidence among the population cannot be determined. This is due to the fact that many more people were infected than tested. Another study also found that the incidence of myocarditis had not increased among young people until May 2021, i.e. until vaccination. If myocarditis occurs after Covid-19, it happens in older patients with comorbidities.
Another autopsy study shows that myocarditis should be included in the analysis of Covid-19 vaccination and mortality. In both the short and medium term, myocarditis can certainly contribute to excess mortality.
As far as thrombosis is concerned, the signals are less clear and, in any case, strongly related to other risk factors.
After a brief discussion of the innate and adaptive immune system, it is explained that the innate immune system is also affected by vaccinations, sometimes for the better but sometimes not. In that case, defences against other diseases weaken. As yet, this is not addressed in the introduction and registration of new vaccines. Studies show that Covid-19 vaccinations but also the disease itself have effects on the innate immune system.
There are many conceivable mechanisms by which the Covid-19 vaccines could contribute to excess mortality. The authors criticise the registration trials and propose a feasible monitoring method that could very quickly signal whether an adverse reaction is associated with vaccination.
Chapter 9 – Conclusions and recommendations
The excess mortality itself is not up for debate. Statistics such as those described and carried out in this report make a certain causal relationship between Covid-19 vaccinations and mortality plausible. Research into the relationship between vaccines and mortality is necessary, given the circumstances. It has been made clear that it is no longer sufficient to point to previous studies, including those by RIVM/CBS and data from the EMA. We have seen no signs in either our micro- or macro-analyses that vaccines have ultimately provided real protection against overall mortality.
Lack of transparency is crippling not only for the vaccination programme but for science in general. This will require a different handling of data.
We have made it sufficiently clear with this report that the Covid-19 vaccines are probably not at all ‘safe’ and ‘95% effective’, as successive health ministers have claimed as a mantra for a long time. The Dutch media, with several science journalists in the lead, have so far seized on everything to ridicule a possible suspicion of the vaccines in advance.
Therefore, this is the most important thing: ensuring that further research into the data and safety of vaccines is normalised. This report is as transparent a representation of the current state of affairs as possible, with the knowledge we could gather within our means at this time. We therefore hope that the publication of this report will be able to trigger something along these lines.
Beautiful, readable summary of an extensive work, which is becoming so well known!
Thanks again! Is it an idea to send this summary to the members of the cabinet, the House of Representatives, the Senate and to the parliamentary inquiry into the corona committee! Minister Agema is too personally involved medically because of her chronic illness, which makes it difficult for her, I think. Down with the ostrich politics!
Good, Anton.
Moet bekennen dat ik zelf ook mijn concentratie verloor op een bepaald moment. Het bevestigt wat ‘wij’ allang denken. En ‘wij’ zijn niet alleen natuurlijk, al lijkt dat wel zo als je de MSM volgt. Misschien zitten (in willekeurige volgorde) Meester & Jacobs, Herman Stijgstra, Cees vd Bos, Robert Malone, Dennis Rancourt, Steve Kirsch, professor Fenton, John Campbell, de mensen achter Panda Uncut, John Ioanidis, Jay Bhattacharya, Jan Bonte, Maurice de Hond, Jona Walk, Maarten Fornerod, Aseem Malhotra, Dick Bij, Pierre Capel, Theo Schetters, Blckbx, DNW etc. er allemaal naast. Ik heb nog geen enkele inhoudelijke weerlegging gezien. Alleen maar beledigingen en persoonlijke aanvallen. De grafiek bovenin spreekt boekdelen. Ingewikkelder hoeven we het niet te maken.
Where is the substantive discussion? Maybe a good start seen at Blckbx DWIV with as guest chairman of the NVJ (Dutch Association for Journalism). They disagreed, but in a polite way.
Goeie uitzending van Blckbx, Anton! Eigen parochie natuurlijk, maar wie weet, groeit die.
Dank Cees!
Deze summary trekt fermere conclusies dan M&J doen.
In my opinion, the only tenable conclusions are:
1. There is increased mortality in a cohort if that cohort has just been jabbed.
2. This indicates mortality due to the vaccine, and of course in the vaccinated
3. the HVE in combination with errors in the data ensures that the data shows just the opposite, namely excess mortality in the unvaccinated and under-mortality in vaccinated people. With a very large HVE, the data can even be good! (Anne Laning rightly argued that).
4. We already know for sure that the CIMS is incomplete due to 3% privacy refusers and by deleting records of people who were already deceased at the time of registration.
5. Because the data are incorrect and the HVE is difficult to determine, it is very difficult to determine the VE and mortality of the vaccine.
6. What is certain is that the VE and mortality have been presented far too rosily in previous CBS/RIVM/NIVEL reports on the basis of these data. But how much, we don't know. And it will be very difficult to determine that exactly. Normally, you do that with an RTC with placebo. But in hindsight, I think you can hardly solve this. You would then have to check the files of the deceased and check why they were not vaccinated. Maybe with a large enough sample? Then you can determine the influence of the HVE and with correct (i.e. corrected) other data you can then calculate the VE and the mortality of the vaccine. In short: that will be very difficult.
Thanks Jan, very pure. We're not that far apart. Because the scientific uncertainty was used as a counter-argument in the report, I formulated it more bluntly. It may not be so explicit in M/J at times, but I think it's all defensible with the report in hand.
Dear Anton,
For the sake of completeness, I would like to say this, in order to avoid any misunderstanding. By writing down my thoughts, I also organize them more and more sharply. I think this correctly describes the current state of affairs.
H.2 is decent. But the fact that excess mortality will fade away in 1.5 years is debatable. Anne Laning argues (in my opinion on reasonable grounds) that in view of the time of death and lost QALYs, the under-mortality should be spread over approximately 5 years. So then the expected under-mortality is less and so is the measured excess mortality.
H.3. Investigations by pharmaceutical companies are notoriously rattling....
H.4. De tekst is m.i. te tendentieus opgeschreven door M&J. Ze hadden zich bij data en analyses en conclusies moeten houden en niet over gedoe rondom publicaties moeten schrijven. Dat wekt alleen maar allergie en verdachtmakingen op…..
But the findings (rattling data and rattling definitions/methods) are correct. There is no good evidence for the VE and mortality of vaccines. Because no RCTs have been performed. And the one who had started got sick halfway through (placebos still vaccinated).
H.5. Ook jouw eerste alinea is aanvechtbaar, omdat door een sterk HVE je geen goede uitsplitsing kunt maken van effecten van de prik op wel/niet gevaccineerden. Dat is de crux van de kritiek van Anne Laning. En daar heeft hij m.i. echt gelijk in. Dus hoewel M&J zich bewust zijn van het HVE, houden ze er zelf ook niet voldoende rekening mee tot welke gekke resultaten dit kan leiden (en Maurice is daar m.i. ook ingetuind). Die Laning is een vaccin protagonist, en deels blind, maar hij is niet dom! En heeft dus vaak terecht kritiek op de vaccin critici. En is, terecht, allergisch voor tendentieus taalgebruik van M&J. Maar hij gelooft weer te lichtvaardig positieve publicaties over vaccins. M&J zouden met Laning moeten samenwerken!
The only thing you can conclude is that every round of vaccinations of a cohort with increased mortality coincides in that cohort, without (per cohort selective infections with Corona) being able to explain this. This leaves vaccination as the most plausible explanation.
H.6. Of these, only the following remains:
a. the CIMS database is polluted with too few people with status "Vaccinated".
b. because of the HVE (and missing "Vaccinated people") you cannot make any meaningful statement about the subgroups vaccinated or not.
c. Both artificially matched and crude mortality data show that there is increased mortality in that cohort after a round of vaccinations of a cohort. Breakdown by vaccinated status is impossible due to errors in the data and the unknown value of the HVE. Because there is pollution and increased mortality, the only conclusion you can draw is that reports by CBS/RIVM/NIVEL make overly optimistic statements about low mortality due to vaccines and about the high VE. But how much too optimistic that is, cannot be determined with the current data. And probably not even without further primary data collection of the reason for not vaccinating people (very) (shortly) before their death.
In your description of H.6, this is the only "hard": " The small increases in overall mortality of different birth year groups move synchronously with the respective vaccination rounds. ". Incidentally, this is a very crucial finding!
Maar al je uitspraken over uitsplitsingen in subgroepen zijn niet houdbaar; en ook die van M&J zijn niet allemaal houdbaar.
H.7. generically, the findings are correct. But statements about breakdowns are highly questionable.
H.8 In my opinion, it is difficult to judge in terms of scientificity. I don't think it's the strongest chapter....
H.9.
The only tenable conclusions:
1. Er is schade a.g.v. vaccinatie vanwege synchrone optreden van verhoogde sterfte en vaccinatierondes in overeenkomstige cohorten; maar we weten niet hoe groot die is a.g.v. het HVE en fouten in de data.
2. De door CBS/RIVM/NIVEL gerapporteerde VE is door fouten in de data zeker te hoog. Maar het zou kunnen dat de VE toch positief is.
3. Nader onderzoek kan wellicht uitwijzen of de schade, afhankelijk van de leeftijd/risico groep kleiner is dan de VE-winst. En dus vaccinatie voor bepaalde groepen zinvol is. Maar dat zal niet eenvoudig zijn; niet vanwege de data, want dat lijkt wel te repareren; maar wel vanwege het HVE. Het HVE kan alleen in een RCT uitgeschakeld worden. Achteraf zou het misschien kunnen door alsnog via een steekproef te achterhalen wat de redenen geweest zijn om mensen in hun laatste weken/maanden niet meer te vaccineren en op welke schaal dit gebeurde. Heel lastig dus…..
Dear people, When looking up information about vaccinations in nursing homes, I came across the following: National Institute for Public Health and the Environment rivm.nl Work Instruction Corona Vaccination Institutions with medical service. Received at the same time as flu shot. Vaccinations for children aged 6 months – 4 years and 5 years – 11 years Comirnaty Omicron JN.1 Register subject with text about source system etc. different e-mail addresses including cimsbeheer@ rivm.nl. Sometimes it says private above. Among other things, at page updates and registration. I also came across lci.rivm. And I thought I knew a lot, but it's much worse. They even vaccinate primary vaccination series in children under 5 years of age and then the booster. Folks, stay away from pediatricians with your kids! If there is no other option, find someone who wants to help you without those jabs! Anton, can anyone figure this out? I've used a space here and there so as not to put some who would like to read along on a track... Thanks in advance!