
ASMR is a statistical method that is often used to measure excess mortality. But there are circumstances in which ASMR evens out and dampens the actual excess mortality, for example in an aging population, in an age-discriminatory disease or in a combination of both. In fact, ASMR does not show the actual excess mortality at all. Not at all.
Om achteraf de virulentie van een virus in twee landen met elkaar te vergelijken, moet je die twee bevolkingen zoveel mogelijk aan elkaar gelijk maken, qua grootte en qua leeftijdsopbouw. Met meer kwetsbare ouderen zal het virus immers dodelijker lijken. Het virus is in zo’n bevolking ook dodelijker, maar dat ligt niet aan het virus. Om dat uit te zoeken werk je met ASMR, waarmee je net doet of beide landen dezelfde leeftijdsopbouw hebben. Eigenlijk zou je ook nog moeten corrigeren op lichaamsgewicht, geslacht, kwaliteit van zorg etc., om de kwetsbaarheid van beide landen zo vergelijkbaar mogelijk te maken. Zo houd je alleen de viruliteit van het virus zelf over. Op die manier probeer je dus te corrigeren voor ‘confounders’. Je wil immers alleen viruseigenschappen meten, niet de sterfte. De ASMR-methode is dus niet geschikt om oversterfte te berekenen. Daarover gaat dit artikel.
First the basics
To look at mortality comparisons and developments, we start by counting the number of deaths per period, for example per year. In the Netherlands, mortality is usually almost four times as high as in New Zealand, for example, and that is not surprising because we also have almost four times as many inhabitants.
The first step in comparing countries is therefore to pretend that those countries are the same size and to calculate how many deaths there would have been. That is not so difficult to calculate back, for example per 1,000 or 100,000 (100K) inhabitants. Then you have the Mortality Rate. Those are the last two letters of ASMR.
In New Zealand, it was 7.2 per 1,000 inhabitants in 2024, and 9.7 per 1,000 in the Netherlands.
Then we are still 20% higher. Should we be worried about that? Did the virus have more deadly properties here? And that's where ASMR comes in. An important factor for mortality in a country, we know, is the number of elderly people. If there are many more elderly people in one of the two groups you are comparing, this natural excess age-related mortality will be able to influence your research results. And what does it turn out to be? We have many more elderly people. About 80% of all deaths come from that group. A larger share of people over 70 (almost 20% more) therefore also means a higher national mortality rate.
So if the question is whether people die earlier in our country, the answer is: no. You can make a statistical correction for this by making those groups the same size in both countries, i.e. giving them an equal share in the population, just as you have made the population sizes comparable. You take away the elderly (or add them) and pretend that they have the same population structure. That is more precise (per age), and in the end you add all those age groups back together to arrive at one number.
Met ASMR neem je niet de werkelijke groepsgroottes maar je neemt voor Nederland dezelfde groepsgroottes als (bijvoorbeeld) voor Nieuw-Zeeland. Evenveel ouderen. Et voilá! Nu komen Nederland en Nieuw-Zeeland mooi overeen. Mensen gaan hier niet eerder dood maar we hebben hier gewoon meer mensen in de groep waar de meeste overlijdens vandaan komen. Het virus had hier dezelfde virulentie (ziekmakende en dodelijke eigenschappen). De oversterfte wordt daar helaas niet minder van.
That standardization of age groups are the first two letters of ASMR. "Age Standardized Mortality Rate: you standardize the population structures in your comparisons.
So far so good.
Counting (and predicting)
Suppose that in a certain year we have to deal with a highly age-discriminatory disease. This means that the Netherlands will be hit harder than countries with fewer elderly people. More mortality, much more than expected. So also a higher excess mortality than New Zealand. After all, age is a supporting variable of the effect, this time it is not a confounder that you want to filter out. Seen through the ASMR glasses, excess mortality there is just as serious as here... or just as insignificant. That does not correspond to reality. The fact that the elderly are much more severely affected and that this drives up excess mortality is largely corrected (perhaps just within a 'safe' bandwidth).
Yet that happens a lot. The elderly are filtered out: "Nothing to see here."
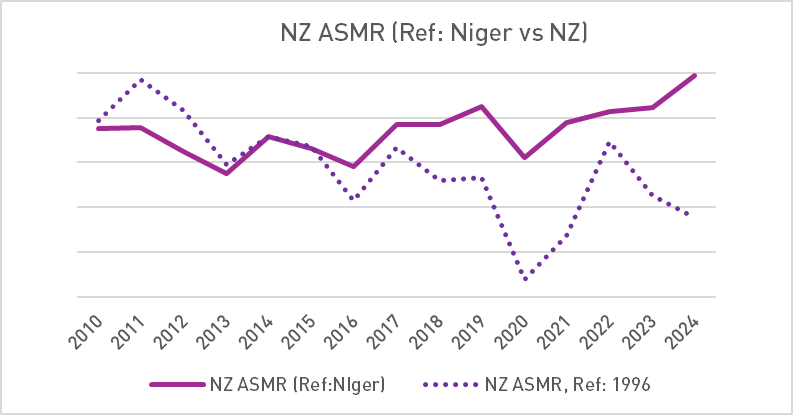
ASMR makes all countries the same age. Let's charge to make it even clearer: a country like Niger has hardly any people over 70, so you can, based on a standard population structure, calculate an excess mortality for that country that is not possible at all, simply because those older people are hardly there. Yet you pretend they are there. In reality, the expected mortality will hardly be exceeded in the event of a highly age-discriminatory disease. Conversely, you can eliminate excess mortality in New Zealand by projecting the population structure of Niger onto it.
The purple line is the mortality in New Zealand, ASMR with Niger as a reference. That line does not reflect the peak of 2022 (see the dotted line). The Mortality Rates of New Zealand are therefore calculated on the basis of the population structure of Niger. The dotted line is the course based on the population structure of New Zealand itself. So what you're saying is basically: if New Zealand had had the reconstruction of Niger, there would have been no excess mortality. (Note also the uptick in 2024: the younger ages are affected.)
In short: If you take a 'standard' population structure with too many elderly people for a specific year, you exaggerate the excess mortality. If you take a standard population structure with too few elderly people, you downplay the actual excess mortality.
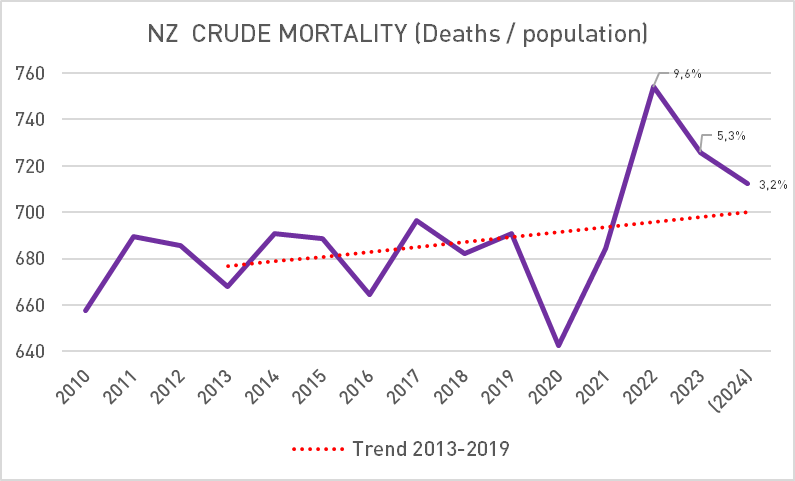
Om de reële sterfte voor een land te berekenen (en te voorspellen) moet je de werkelijke bevolkingsopbouw gebruiken van het jaar waarvan je de sterfte berekent. Zo kom je tot wat heet de “Crude Mortality”. Dat kan andere resultaten geven dan ASMR.
Ageing
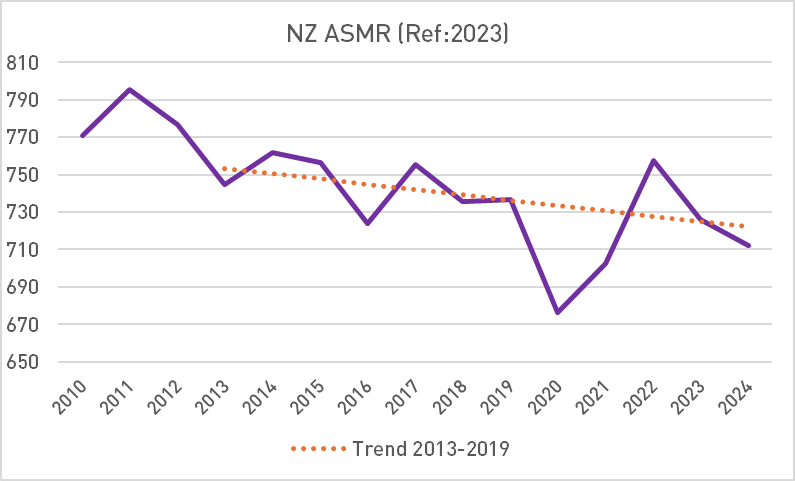
It becomes even more problematic if we start ASMR historically. I'll take New Zealand again. In 2010, the percentage of people over 70 was 8.9%, in 2023 it was 11.5%. You can cancel out that increase of more than a quarter (29%) if you use the same population structure for all years. With two implications.
Take the average as the standard population, for example: 10.2% is 70+. This mathematically increases the actual mortality of the years when there were fewer people over 70. This will make the expectation for the following years, so that any calculated excess mortality in later years will be lower.
On top of that, there is the effect, but in the later years, that in reality there were more people over 70 than are calculated, so in those calculations the mortality was actually calculated too low, which further dampens the excess mortality.
In short: in an aging country, ASMR can be used to increase the forecast (baseline) and decrease the actual number. By definition, this happens in the case of a highly age-discriminatory disease that affects the elderly in particular. Met het handig kiezen van een baseline, beginnend op een ‘laag’ jaar en eindigend op een ‘hoog’ jaar, is in het geval van Nieuw-Zeeland zelfs aan te tonen dat er ondersterfte is. Dat gebeurt dan ook. (Die ondersterfte was er in 2022 overigens niet, toen iedereen gevaccineerd was, maar dat terzijde.)
WHO 2013
The general principle is that a population does not age in the ASMR model, no matter what population structure you take. In a rapidly aging world, this is a method to be alert to. Age-related diseases do not increase when you look through ASMR glasses.
So far, we have used our own model populations. If everyone uses the same standardization, the results will be universally comparable. The WHO has therefore proposed a model population structure: WHO 2000-2025. The effect remains the same: previous years result in an increased baseline when the population ages, and elderly mortality is proportionally less increased as the years go by, sometimes even decreased.
There is also a European Standard Population, daarmee wordt het zo bont niet. De oudere categorieën zijn in dat populatiemodel ruimer vertegenwoordigd dus van een verlaging van de sterfte zal het niet gauw komen, alleen van een geringere verhoging in vergrijsde jaren dan in jaren daarvoor, maar dat heeft een soortgelijk sterftedempend effect.
Let's assume for a moment that the proposed European standard population accurately reflects the EU population. So, for example, the Netherlands has almost exactly the average build-up. Purely hypothetical. In that model population, 5% consists of people aged 80 and older (and that happens to be the case in the Netherlands as well). This group contributes more than half to total mortality and traditionally even more to excess mortality.
Then we will ASMR with WHO 2000-2025. It has only 1.54% of people over 80. So we are going to pretend that the Netherlands does not have 5% but 1.54% of people over 80. The group that accounts for half of the mortality will be reduced by 70%. That means: 35% less mortality in the Netherlands after ASMR with the WHO-standard world population. I don't think it's a good idea to use that alone to interpret excess mortality quantitatively.
In fact, if someone wants to launder or downplay excess mortality, this is certainly a method that can help. So now you know what it means when a CBS spokesperson says: New Zealand has been heavily vaccinated and there we do not see any excess mortality in an age-standardized way. Or that you can only trust numbers if they have been ASMR'd.

Vaccine damage and ASMR
Wolfgang Wodarg exaggerated in 2021(!) when he said that all deaths came from 5% of batches1https://virusvaria.nl/berichten-uit-de-onderwereld/#:~:text=Mijn conclusie.-,Bad batches,-Een ander bericht. It took two years for German scientists to map it out more thoroughly: half of the death reports came from 5% of the vaccine batches2https://virusvaria.nl/de-helft-van-de-oversterfte-komt-van-5-van-de-vaccinbatches-zeggen-duitse-wetenschappers/. This still indicates unprecedented and unacceptable product instability. When these differences were identified, the first reflex was: "These must be the batches that have ended up with the vulnerable elderly. It is logical that you see more mortality there because it cannot be due to the vaccines."
We recognize the ASMR argument here. And it's also interesting: is the effect age-dependent? This has been investigated: age did not appear to explain the differences.
Later, bad batches were found to hit much harder in Denmark than in Sweden3https://virusvaria.nl/onmogelijke-batch-cijfers-vs-denemarken-zweden-tsjechie-belgie-nederland/. De onderzoekers hadden al bekeken of leeftijd ermee te maken had: dat was wederom niet zo. Het product is gewoon instabiel en ergens in de keten lijkt een variabele te zitten waardoor het fout kan gaan. In dit specifieke geval kan het ook nog zijn dat de Zweden beter bestand waren tegen de toxische spikes. Daar was het virus immers al goed rondgegaan en dat heeft mogelijk bescherming tegen de vaccins opgeleverd.
Theorem
In a highly age-discriminatory disease such as Covid-19, ASMR allows you to change facts that are supporting variables of the subject you want to look at. In aging populations, ASMR acts as a dampener on excess mortality, whatever static distribution is taken as a reference, because the growing number of elderly people is ignored. Crude mortality gives a realistic picture of this. If you calculate excess mortality Crude, not with ASMR, you get "ASMR excess mortality", which is based on mortality probabilities and not on the difference between expectation and reality.
With ASMR you compare the properties of the virus or mortality rates – but what you don't measure is the degree of excess mortality. ASMR is useful and educational – but you have to be careful because sometimes the method is not performed by accident...
References
- 1https://virusvaria.nl/berichten-uit-de-onderwereld/#:~:text=Mijn conclusie.-,Bad batches,-Een ander bericht
- 2https://virusvaria.nl/de-helft-van-de-oversterfte-komt-van-5-van-de-vaccinbatches-zeggen-duitse-wetenschappers/
- 3https://virusvaria.nl/onmogelijke-batch-cijfers-vs-denemarken-zweden-tsjechie-belgie-nederland/
Thank you again for your efforts and info, but have you ever looked at TKp.at and The Expose, especially at TKP.at you will discover a wealth of research/results, highly recommended!
Hello Ron, I know these news sites but don't follow them daily. Fortunately, there are such alternative news sources that dare to report what is not on TV.
Very clear, thank you!
I already realized that ASMR can sometimes be misleading, but now I realize that much better.
Fine! It was quite a challenge to explain, at least it seems to have 😊 worked out reasonably well
ASMR is a tool for me, to compare countries (slightly) more easily. But certainly not the ultimate indicator.
Comparing countries with ASMR, and then going into depth, if it turns out that a country scores 'better' on certain components.
Isn't it better to just look at the average age of death for men and women? If it drops, then there is certainly something wrong. If it rises, it is positive. In the USA the average age is dropping, although I read somewhere. So that's not okay. Isn't this more important than the number of people who die?
LE (life expectancy) is directly linked to mortality.
In addition, we see that life expectancy for women has been stable for years. For men, it still increases slightly. But they were already lagging behind.
As Bonne says, it doesn't matter, another way of expressing the same thing.
Thank you for this explanation about asmr. Very complex for a layman, but with this explanation I think I roughly understand what is explained in the publication of 12-4-2025. It doesn't change the fact that we are being fooled.
This is another good example that you have to be very careful with models.
It is much better to "just" publish and benchmark the (under) mortality per age group.
No one can ignore that. Because no tricky edits have been unleashed on it.