
Just after corona made its appearance in Europe and the Netherlands, Frank Ruesink, himself the father of a child with vaccine damage, had a short conversation with Hugo de Jonge about alternative solutions to combat the corona virus. Hugo de Jonge's answer to Frank Ruesink's question whether these alternatives would also be looked at was: 'I certainly wouldn't count on that. Vaccination is really the only thing that really helps...' (see here the excerpt).
It was clear from that moment on that the government in the Netherlands, as in many other countries, had put all the cards entirely on vaccination as the only way out of the corona epidemic. Governments around the world donated billions of euros and dollars to science to develop vaccines as quickly as possible. In many news broadcasts, the population was kept informed of developments, trials and initial research results.
Meanwhile, skeptics, including many scientists and experts, pointed out a number of potential pitfalls in this strategy. However, if they shared critical voices, they were often treated aggressively on social media and not long after even censored on Big Tech platforms such as YouTube, Facebook and Twitter. Criticism of vaccination was dismissed as 'wappiepraat', 'conspiracy theory' or ridiculed with comments such as 'are you suddenly also a virologist'? A mature conversation in which arguments and results of studies were exchanged was, and in many cases still is, impossible.
In this article we look back at the content of the criticism, and whether this criticism was justified or not.
Four criticisms
- The first criticism of the vaccination strategy is that in the past it has never been possible to develop a vaccine against a coronavirus. One of the reasons is that during the development of the vaccine, a phenomenon occurred called Antibody Dependent Enhancement. In laboratory animals that received a corona vaccine, more serious symptoms developed after vaccination and confrontation with a wild type of coronavirus than in unvaccinated laboratory animals. In other words, vaccination made the test animals more sick than it protected them. In trials with children, this even led to the death of two children. This has been discussed by, among others, Dr Peter Hotesz, one of the leading scientists in the field of vaccinology in America.

- The second criticism of the strategy is that developing a vaccine for a coronavirus is not possible, because the virus itself mutates quickly. As a result, a vaccine that offers defense against a variant, for example the Wuhan variant, can very quickly lose its effectiveness with the emergence of a new variant, such as Delta or Omikron. Piere Capel, professor of immunology, was one of the experts in the Netherlands who pointed out this danger.
- A third point on which the strategy has been criticized is that the vaccine triggers an immune response from the body, but that this reaction in people with a weakened immune system (such as vulnerable elderly people) can therefore only generate a small amount of protection. After all, the vaccine depends on the human immune system in order to reactivate the immune system in the event of a subsequent infection on the basis of the earlier infection experienced by the vaccine. This criticism mainly focuses on the effectiveness of the vaccine for the people who need it most. For these people, by definition, the vaccine would not work as well as for the people who need the vaccine less at all, because their immune system is strong enough to be able to beat the virus without a vaccine. One way to determine whether a vaccine is effective is to calculate the relative risk reduction of the developed vaccine for the various age or risk groups.
- Finally, there was also a lot of criticism of the technique used of the vaccines in combination with the fast development time, and therefore a short time for conducting studies on the safety of the vaccine. Pfizer and Moderna, have developed their vaccine based on mRNA technology. This technology has previously been used in cancer treatments, but has never been widely used for vaccination. With this technique, the cells in the body receive an RNA instruction to make a protein that also occurs in the virus. This protein is then placed on the cell wall by the cell, after which the immune system recognizes it as a protein from an intruder, and sets to work to clean it up. The idea is that not the whole virus is injected, but the instruction for creating a characteristic part of the virus. Corona is about the spike protein. Critics pointed out that if the vaccine enters the bloodstream, it can then go to all kinds of cells, after which the body starts attacking the cells in which the protein is expressed, which can lead to inflammation, but also autoimmune diseases, or even the accelerated development of cancer.
Evaluation of the criticism
We can now see in chronological order whether the criticism was justified.
In September of 2020, the first results of the pfizer and Moderna studies came out. They claimed that the corona vaccine was more than 90% effective. The news was met with cheers. At least, by almost everyone. Experts who read the research results a bit better came to the conclusion that Pfizer's research design was insufficient to assess effectiveness. For example, Peter Doshi, associate editor of the BMJ (a renowned scientific journal) indicated that the design of the study should be such that it assesses whether it prevents people from becoming seriously ill, ending up in the hospital or dying and also whether the vaccine stops transmission. This was his conclusion after reading the study design:
‘None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.’
https://www.bmj.com/content/371/bmj.m4037#:~:text=Hospital%20admissions%20and%20deaths%20from,not%20designed%20to%20find%20out.
Once the vaccines were on the market, an article in the Lancet calculated how effective the vaccine really is. The authors conclude that absolute risk reduction (ARR) of the vaccine is very low. The absolute risk reduction is the decrease in the chance that you will get sick based on the chance that you will get sick before you have taken a vaccine. Based on the study results, the authors of the article arrive at the following results for Absolute Risk Reduction:
“ARRs tend to be ignored because they give a much less impressive effect size than RRRs: 1·3% for the AstraZeneca–Oxford, 1·2% for the Moderna–NIH, 1·2% for the J&J, 0·93% for the Gamaleya, and 0·84% for the Pfizer–BioNTech vaccines.” (https://www.thelancet.com/journals/lanmic/article/PIIS2666-5247(21)00069-0/fulltext)
This shows that for the people who have little risk of getting severe covid, vaccinating actually makes no sense at all. The effectiveness of the vaccine is really only in the groups that have a chance of severe covid, and from data worldwide and from the Netherlands we know that this chance is only starting to get serious in the group of 70 years and older. Worldwide research by Professor John Ioannidis has shown this: https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.13554
Despite this criticism, around the end of 2020, the Western world has started the mass rollout of vaccines. First a dose, but soon a second dose. With this, the general public expected that the epidemic was over and lockdowns, one and a half meters and face masks would become a thing of the past.
In 2020, several mutations of the coronavirus emerged. Logical, because the virus mutates quite a bit. This can be seen here: https://nextstrain.org/ncov/gisaid/global. So we were confronted with the British variant, the Brazilian variant, the South African variant and the Indian variant. These variants were later renamed and have been given Greek letter names. Now these variants are better known as Alpha, Delta and Omikron. And with the arrival of variants, we also got 'waves' again, despite the high vaccination coverage among the elderly and to a lesser extent among the younger age groups.

Soon it became clear from data and research that the vaccine does not stop transmission (source: The Lancet) and even that a naturally experienced infection offers better protection than protection provided by the vaccine, also in The Lancet.
This is in line with points 2 and 3. After all, the immune system that has defeated the entire virus recognizes in a subsequent confrontation with a mutated virus the parts that have not or hardly mutated. This cross-immunity was known fairly quickly in 2020 that it offered protection against the new coronavirus.
So far, it has been shown that criticisms 2 and 3 were justified. What about points 1 and 4?
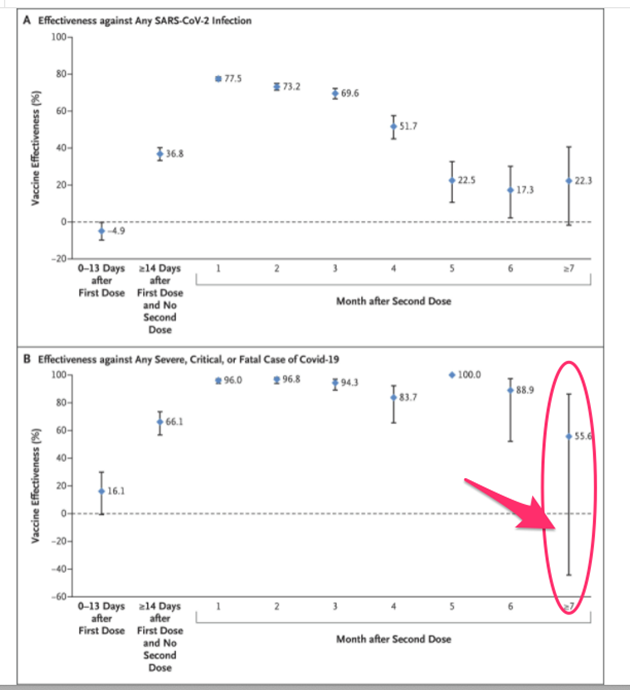
For a long time, the existence of ADE with this corona vaccine has been denied. In fact, this summer, several countries were simultaneously talking about a 'pandemic of the unvaccinated'. Vaccinated people would not or to a much lesser extent end up in the hospital or in the ICU. In some countries, however, the researchers saw something striking: after a few months, the protection of the vaccine seriously decreased and after 7 months the protection even became negative. Could these be the first signs of ADE or similar mechanisms?
From research in Qatar it can be seen that protection becomes negative after 7 months.
In the meantime, there was a discussion in the Netherlands about the percentage of people vaccinated in the ICU. This discussion raged mainly in the autumn of 2021, but quickly faded when figures, including from the CZA, showed that the percentage of vaccinated people in the hospital rose rapidly.
Remarkably, Hugo de Jonge and the RIVM did not want to share figures about the ratio, and in January 2022 no one is actually talking about the pandemic of the unvaccinated anymore. Not in the Netherlands and not abroad. In fact, Pfizer's CEO now indicates that two doses of the vaccine do not or hardly protect, something that was unthinkable to say in mid-2021.
Very recently, however, research has come out showing that due to the emergence of the last variant, the Omikron variant, vaccinated people are not less, but MORE at risk of infection. With this, the whole story of vaccination protection falls apart completely. Conclusion of a study from Canada:
'Our results demonstrate that the effectiveness of 2 doses of COVID-19 vaccines against infection (irrespective of symptoms or severity) is substantially lower for Omicron than Delta, and that VE against Omicron infection was only 37% ≥7 days following a third dose. We also observed negative VE against Omicron among those who had received 2 doses compared to unvaccinated individuals.'
https://www.medrxiv.org/content/10.1101/2021.12.30.21268565v1.full
It seems that now more and more studies show that people who Vaccinated are a greater chance run on infection with a new variant than unvaccinated people.
Much has been written about collateral damage on this website, including about myocarditis, excess mortality, and the large number of reports of side effects in VAERS and lareb. The latest news is about inflammation of the spinal cord and swollen lymph nodes after the booster:
From the news of January 14, 2021:
“EMA: rare spinal inflammation possible side effect of vaccines Astra and Janssen
According to the European Medicines Agency (EMA), a rare inflammation in the spine is a possible side effect of the corona vaccines from AstraZeneca and Janssen. The neurological disorder myelitis transversa can cause, among other things, limpness in arms or legs, tingling, numbness, pain and problems with the bladder and intestines.
People who have received one of these vaccines and who are getting these symptoms are advised to seek medical attention immediately. Health care providers should be alert to signs and symptoms of transverse myelitis, writes the EMA.
An EMA research group concluded that a causal relationship between these vaccines and transverse myelitis is "at least a reasonable possibility.". However, the advantages of the vaccines far outweigh the disadvantages." (source: nos.nl)
"Every day, the Lareb Adverse Reaction Centre receives dozens of reports of swollen lymph nodes after receiving the booster shot. And that is striking, says director Agnes Kant to RTL Nieuws. That is why the reports are currently being investigated."
Source: RTL News)
We can conclude that the critics have been proved right on all four counts now, two years later. Due to the failure of stopping the epidemic by the vaccine and the rise of Omikron, it can be definitively said that the government's vaccine policy has ended in a complete flop.
