
In the healthcare industry, everything revolves around the patients, but once they have passed away, the deceased are not exactly treated with respect. At least not at the top of that industry. And certainly not if a link could be established between death and vaccinations. This already started in the Pfizer trials and we now also see it in the Dutch government's approach that makes excess mortality disappear from statistics.
RIVM in transition
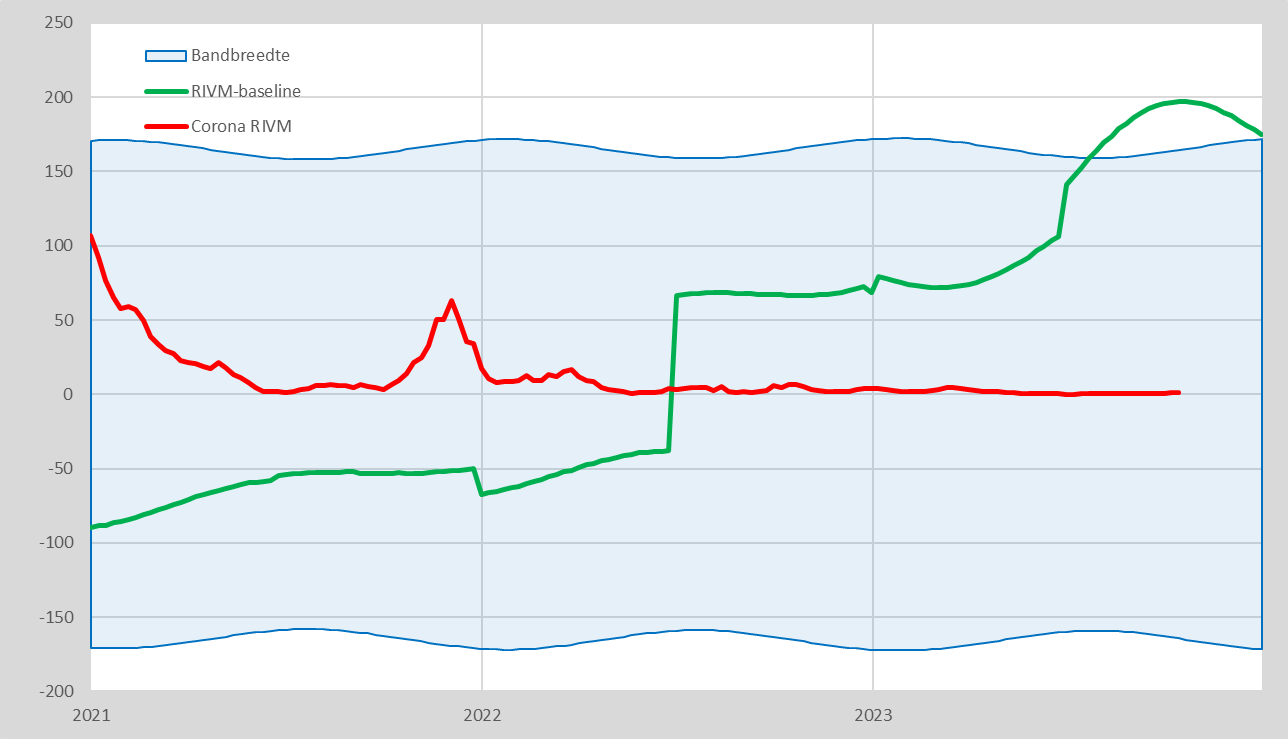
As previously reported, RIVM is taking over the monitoring of mortality from CBS. Strangely enough, this is reason for RIVM to gradually increase its own old expectation level. We compare the new RIVM baseline with the usual baseline of CBS. What stands out? I took some elements from Herman Steigstra's graphs.
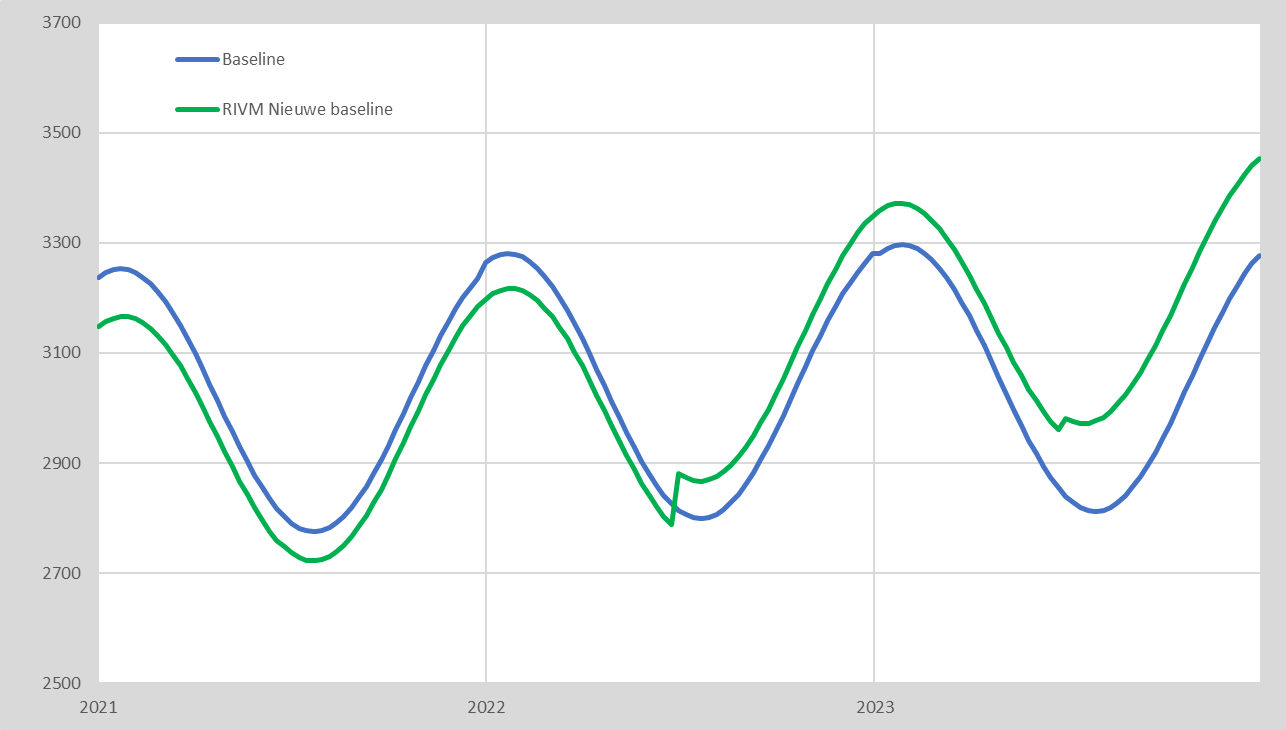
- It may have escaped your notice, but as of mid-2022, Dutch people have died on average a few months earlier than previously expected, which will be extended to a 5-month shorter life for the average Dutch person by the end of 2023. So we are heading towards half a year shorter life and maybe our life will be shortened even further. Cause? Unknown, or rather: unexplained. We are curious to see what this will mean for insurance and pensions.
- The RIVM forecast starts three years ago. The forecast for 2021, which was previously calculated by CBS, has therefore been adjusted downwards with retroactive effect. Why don't they start at the level where CBS stopped? I see two options:
- The starting point had to be in line with the existing expectations of RIVM, otherwise it would seem as if they had been too low all these years. So there had to be a bridge between the old RIVM baseline and the new, increased expectation.
- A lower forecast for 2021 means that excess mortality in 2021 will turn out to be higher than expected. There was still some Covid mortality at the time. In the past, CBS has attributed all excess mortality to Covid, including in 2021. If that remains the case, even more excess mortality could now be attributed to Covid.
- From mid-2022 there will hardly be any corona deaths. There, the mortality expectation is increasing and excess mortality is therefore being systematically eliminated. In mid-2023 we will see another jump upwards and the increase in expectations will also continue. It will seem as if excess mortality disappeared together with corona...
The National Institute for Public Health and the Environment (RIVM) considers the permanently elevated mortality to be a fait accompli and includes it in its mortality forecast for the coming years. In itself, this is defensible, because the RIVM wants to be able to identify occasional flu peaks and heat waves. This is not possible if mortality is always above the signal level anyway.
Dat het RIVM zich niet meer bezighoudt met de postvax-meersterfte is eigenlijk een blessing in disguise. Deze problematiek was ze een maatje te groot. Foute modellen (volgens @dimgrr "de methodiek van de Drie Dobbelende Chimpansees™ "), foute maatregelen, verkeerde prioriteiten, onwetenschappelijk gedrag, om maar wat te noemen. Laten zij zich inderdaad maar met griep en hittegolven bezighouden, daar zijn ze beter in.
This does not alter the fact that the excess mortality that has now been calculated Unexplained remains, even though it is no longer called excess mortality. It is now 'expected' or 'normal' mortality, in the view of the RIVM. However, in the interest of public health and the government's duty of care, it is important to keep an eye on unexplained mortality and to find out where it comes from. The government fails to do this, while this concerns tens of thousands of deaths, especially over the years, including proportionately fewer people over the age of 80.
Conclusions
- It is necessary to also keep track of the real baseline and not to confuse it with the expectations of the RIVM. This is to prevent the entire 'unexplained excess mortality' item from disappearing from the agenda, including the vaccination cesspool where the lid can no longer be kept on.
- We zullen ook onze terminologie moeten aanpassen. We spraken altijd over "onverklaarde oversterfte". Dat wekt verwarring omdat die onverklaarde sterfte vanaf nu verwacht wordt door het RIVM en dus in hun ogen geen oversterfte meer is. Het moet dus vanaf nu in RIVM-termen vermoedelijk "onverklaarde sterfte" worden in plaats van "onverklaarde oversterfte".
So:
- Expected mortality is the total number of expected deaths for next year (and further ahead)
- The baseline is het aantal toekomstige overlijdens, berekend op langetermijn trends in demografische gegevens. Dat is naar ons idee de enige echte baseline en die kan afwijken van de verwachting. Mocht het RIVM echter ook het woord baseline gebruiken voor hun verwachting op basis van recente ontwikkelingen, dan zullen wij moeten spreken van de "virusvaria-baseline" om het onderscheid duidelijk te houden
- The unexplained mortality may or may not be included in the forecast and, depending on this, is either 'unexplained mortality' or 'unexplained excess mortality'.
- The RIVM forecast includes the unexplained post-vax mortality increase in the calculation
- The Virusvaria baseline still considers the anticipated aftermath of the post-vax mortality as excess mortality. We therefore do anticipate additional mortality, but in the form of excess mortality above (our) baseline
- The bandwidth is a tolerance for deviations from baseline or expectation
- The bandwidth can be determined with or without seasonal peaks
- Just like RIVM, we opt for a fairly constant bandwidth (this is different from what CBS did; they were concerned with a correct expectation, not with signal values)
- Increased mortality is the number of deaths above the baseline. (For the RIVM: above expectations).
- Excess mortality indicates bandwidth overruns
- Unexplained mortality is the total mortality minus the baseline minus incidental declared deaths, such as influenza and heat waves.
The term 'unexplained excess mortality' will therefore disappear from the RIVM terminology, which will become 'unexplained mortality'. After all, it is no longer 'excess' mortality for them: after all, they expect it and therefore abandon the traditional baseline. We also see that they overestimate future excess mortality, and a declining trend is already visible. The RIVM will therefore show undermortality in the coming years. This will eliminate excess mortality, bring everything back into balance and ensure that the excess mortality figures are neatly averaged out over the years.
So much for this evaluation of the deletion of deaths. But even in the trials, every effort was made to keep mortality out of the picture. What happened in that trial, namely the fiddling with possible vaccine-related deaths, appears to have had a high predictive value. Too bad it wasn't reported.
Pfizer forgot two body bags
In een brief aan de procureur-generaal van Texas, Ken Paxton, toont Dr. Jeyanthi overtuigend aan dat Pfizer niet alle sterfgevallen tijdens hun COVID-19 vaccinproeven heeft gerapporteerd aan de FDA. Die realiseerde zich dat de Emergency Use Authorization (EUA) daarmee in gevaar zou komen. Als deze sterfgevallen wél gemeld waren, was dat een verdubbeling geweest van het aantal overlijdens onder gevaccineerden. Dat had dan laten zien dat het BNT162b2 mRNA COVID-vaccin de sterfte niet verlaagde zoals oorspronkelijk werd geclaimd ("The benefits outweigh the risks"). Het aantal sterfgevallen in de placebogroep was dan immers gelijk geweest aan dat onder de proefpersonen.
In addition, both unreported deaths involved heart failure, which, according to the researchers, could not be directly traced back to participation in the trials. This raises questions about the reliability and ethical aspects of the reporting process, Kunadhasan writes.
He backs this up with FOIA (WOO) documents, which Pfizer said it would not be able to provide for another 75 years. That wasn't right.
It is to be hoped that Tony Fauci was not informed about this, not even informally, although I am not ruling anything out.
Dr. Jeyanthi Kunadhasan is an anesthetist and perioperative physician in Australia. He examined the data released on the Public Health and Medical Professionals for Transparency website, which formed the basis for the emergency use authorization (EUA) of Pfizer-BioNTech's BNT162b2 mRNA COVID vaccine by the FDA. He is also treasurer of the Australian Medical Professionals Society and co-author of several other reports.
Read the full letter at dailyclout.io

RIVM , batch number -, vax deliten,
You can look it up until 31-01-2024 DigiD
Excellent explanation of the necessity and the terms used in the new Sterftemonitor.nl by Herman Steigstra in collaboration with Anton Theunissen.
On the last sentence: Was Tony Fauci aware? He was one of the originators of the whole Corona Pandemic deception.
It also helped with all vaccine approvals that Ms. Fauci sits on one of those FDA authorization committees.
Is it not now important to pay extra attention to the changes in life expectancy of the population? If, with the RIVM methodology, an under-mortality trend occurs while the average life expectancy is decreasing, it seems to me that this – at least – requires further investigation, because it seems anti-logical.
By the way, if life expectancy decreases even at 67+, the retirement age can be adjusted downwards again, right?
With all due respect, but can't it just be that RIVM and possibly CBS have been messing around with numbers for years and that they are tackling this Corona shit to correct all the data blunders of recent years? I have been working for the government for 30 years and I have never caught them with a healthy data policy, processing or analyses. (I also provided CBS with self-made figures for a number of years because they asked for figures that we could not possibly provide, but were obliged to provide them every year. Not once was an audit carried out or an inquiry made.) In the government they call it an analysis if you repeat numbers in text that graphs directly display. In scale 13 (> tons) the specialists do not even know the difference between a percentage and a ratio or an average. I am sure that the figures surrounding Covid were massively full of errors that of course suited these authorities very well. The primary reason that governments do not look back or want to analyze is because they never really prepare anything through a simple analysis, survey or even reading old documents about projects where the same thing has been tried before. 9 times out of 10, policies are simply created ad hoc based on the issues of the day. When a good person leaves the government, all knowledge, experience and data on disks of this person are deleted and reset to zero. As a rule, no transfer of function and/or knowledge takes place. They don't even have a decent database containing all legislation. Or a search engine that leads you to the correct legislation. Everything is purely amateurish and people are on average 30 years behind developments in ICT. Oh, the IT is modern, but it is completely separate from the work processes, they see IT as a facility service and not as something that should be an essential part of the work processes. They assume all kinds of things in terms of knowledge, but as soon as something complicated is shown by that new recruit, then 1+1=2 then the managers press a panic button and hire expensive agencies that take advantage of this ignorance and then further disguise and obscure everything for their own gain. Good incoming knowledge has left within 3 years. I see every day that incompetent specialists and managers who have been in office for too long seriously hinder progress in government. As long as that problem exists, our country will go from crisis to crisis and Bill Gates and Schwab can continue unchecked. In the land of the blind, the one-eyed man is king.
OMT member Menno de Jong will succeed Jaap van Dissel as Director of Infectious Disease Control at RIVM. Already showed himself in favor of mandatory vacccination against Covid. This does not bode well, because in this new position he will also become an important advisor to the government in health policy. https://www.at5.nl/artikelen/212226/viroloog-de-jong-nadenken-over-vaccinatieplicht-om-uit-lockdown-te-komen
And Menno de Jong's wife also has a position that doesn't make us happy, I heard in a weekly news on an important video channel. There I heard and saw (with evidence) that Marc v R from Belgium also recommended HCQ with a study that it could indeed help in the hospital because there were fewer deaths in the group that received the drug than in the group that did not receive HCQ. I don't know what the protocol was in Belgium. A question for the parliamentary inquiry "What were the protocols in ICUs in 2020 for people with a severe covid infection?" "What dosage of HCQ and other agents?" Kind of. Folks, check your tires before you ride, but don't be scared and also support blckbx.
It is a small world (let's just say clique) from which the RIVM directors are selected. Newly appointed director Menno de Jong comes from the AMC. He worked at the LUMC for many years, where he worked together with Jaap van Dissel – until next April. Director of RIVM – was in the same department of Infectious Diseases. Menno's wife Constance Schultsz, also works on Infectious Diseases at the AMC. And Van Dissel's predecessor at the RIVM was Roel Coutinco, who came from... the AMC Department of Infectious Diseases.
It's like co-optation, in that world of Infection Fighters!
The Ethical Skeptic signals a similar increase baseline in the states. https://twitter.com/EthicalSkeptic/status/1746685316465852776