
When a new mutant appears, all alarm bells ring. Usually the virulence (pathogenicity) of a virus develops in reverse to its contagiousness, but that is by no means certain. So it's important to be on top of it. If Marion Koopmans still says after several weeks: we have to wait for the results, why doesn't she look up Ourworldindata. There, after only two or three weeks (at the end of November), it turned out that omicron was very likely good news. Treating doctors confirmed this. I know: that's not science, but do we still not realize that the country is in crisis?
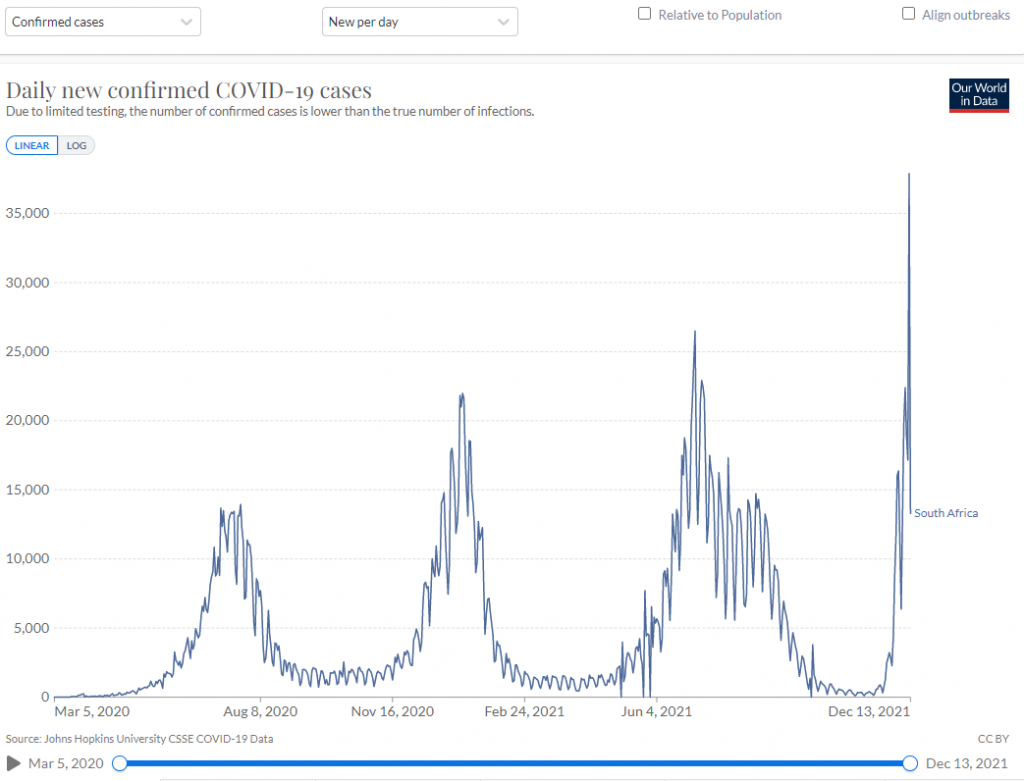
In the top graph you can see the number of confirmed Covid infections. That was the highest ever measured on December 11: 37,875 cases. One and a half times more than the highest peak so far on July 3. The small graphs below show the number of covid deaths per million inhabitants and per confirmed infection: there is no escape, mortality has completely collapsed. Nature has given us a vaccine against the stranger, very likely artificial adaptation in a virus that has brought a lot of misery. But there is even better news. Read on.
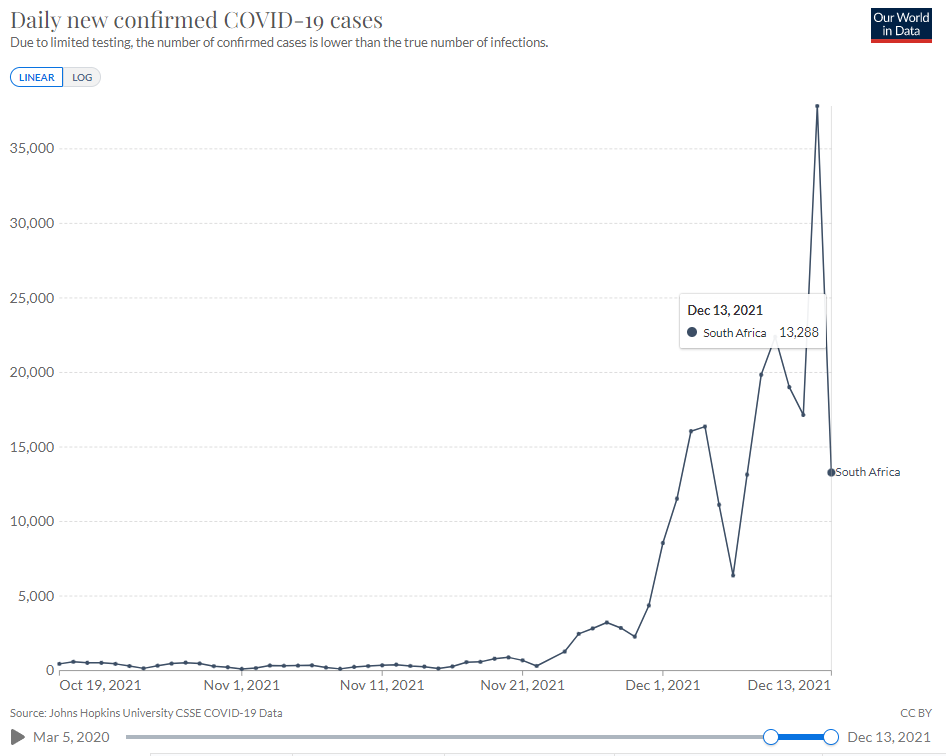
Surprise in the daily figures?
Zooming in on the last few weeks, you see something hopeful – although it is still early to draw definitive conclusions, but still: the Monday report is not 30% lower this time but 65% lower, from 37,875 to 13,288. There will undoubtedly be some more pluses, but if this is the start of a trend, South Africa has reached an important degree of immunity. That took six weeks (Omicron saw the light of day there around November 1). In the Netherlands it can take longer, especially if we close schools, for example, so that children infect grandparents instead of each other. On the other hand, 2G and 3G indoor events can speed up the process a bit. In that respect, we have to wait and see and pay particular attention to Herman Steigstra, who indicates the day cjifers in the Netherlands.
Omicron concerns
The Netherlands has a major problem with its Eastern Bloc care capacity. In our country, deaths are therefore less important than pressure on healthcare; All sensors are aimed at the latter, excess mortality has so far been a side issue. So what about the healthcare pressure in South Africa?
Hospitalizations South Africa

Hospital admissions: still rising – but how far will that continue? (Note: These are positive tests of ALL Covid hospitalizations (with and through), not necessarily real Covid patients)
Mortality in South Africa

No figures are available for ICU occupancy. If we can assume that there is a relationship between ICU admissions and mortality, the ICU occupancy will also be very low. (Keep in mind that there is a week's delay between admission and ICU.) This is also consistent with the image that the hospital admissions are not exclusively Covid patients but also asymptomatic and mildly infected people, who have been admitted for something else but tested positive.
Mortality in South Africa and the Netherlands

South Africa and the Netherlands: number of covid deaths per million inhabitants If you see this graph, you wish you could bring the virus from South Africa into the country.
CFR South Africa and the Netherlands

South Africa and the Netherlands: number of covid deaths per confirmed infection
This seems nice, but it doesn't have to be: the CFR (mortality among Covid patients) has always been much higher than ours. Maybe it's more difficult for us to get it down further, because we already do it so much better. Of course, we hope that it will be decimated with us as well. That leaves only the unexplained mortality, which is then 30 times as high as the Covid mortality.
Recent post from South Africa: Dr. Angelique Coetzee
Dr. Angelique Coetzee talks about the seriousness of Delta and the relief after seeing Omicron cases. She says that the boosters make sense if they not(!) are obliged to be offered to people who cannot afford to get any form of Covid. I don't know how to find out, unfortunately we don't have a reliable source for that in the Netherlands yet. After all, the vaccination is seen as a 'if it doesn't help, it doesn't hurt' injection, which means that no clear balance can be made between benefits and known, unknown and denied disadvantages in the short term and the largely unknown disadvantages in the longer term.