
Ivermectin has been prescribed billions of times, mainly against river blindness. The (limited) side effects are known and doctors know them very well, as do pharmacists. It is a well-known medicine. It is also used as a precaution (prophylactic) prescribed to healthy people who want to travel to Africa - so the side effects are no reason not to do so. Whether you prescribe for river blindness or a lung infection makes no difference to the side effects. You would say that not being allowed to prescribe because of the side effects, under penalty of € 150,000, is a penalty that should prevent a major danger. But what danger is that?
Because river blindness is a disease that is common in Africa and causes enormous damage to health, travelers to Africa are also prescribed Ivermectin. They must take this in advance and, in the case of a 'long stay', during their stay in Africa. Such a stay can last many times longer than a Covid infection. You wouldn't say he can't be in that. The African population will have to swallow it for decades to come to eradicate the disease - or if all goes wrong, forever. That's billions of pills.
River blindness, how bad is that?
In 2005, it was estimated that 40,000 new cases of river blindness occur annually. This left 300,000 blind and 500,000 visually impaired. In some areas, 2% of the population is blind. Adults lose sight over the age of 30. Life expectancy decreases by 8-12 years. (Nature, 2005)
About the Ivermectin program
River blindness is not equally prevalent in all African countries. That may be why a number of countries do not have an Ivermectin program and a number of other countries do. The drug is now also used against malaria: it kills the mosquito that sucks the Ivermectin into the blood.
An Ivermectin program means that everyone receives an Ivermectin pill every six months. It would therefore be illuminating to compare the non-Ivermectin countries with the countries that do have an Ivermectin program. After all, if the drug does not work against Corona, as some 'corona reporters' headline in national newspapers, then you should see no difference between countries with and without an Ivermectin program. Virusvaria reader André de Jong put me on the track.
IVM group and control group
I have found 23 African countries where Ivermectin is used, the IVM group. There may be some errors in that composition because the WHO website is not super clear; some countries joined in later or are in a malaria program with IVM, so please bear with me. It doesn't matter much for the overall picture.
There are 34 countries in Africa WITHOUT an Ivermectin program. For the sake of readability, we call this the 'Control Group'.
Absolute numbers
First, in RIVM style, a comparison of absolute numbers, which is the easiest to understand (if Jaap van Dissel were to read along):
- In the Ivermectin countries, nearly 14,400 Covid deaths have been recorded
- 95,700 were registered in the control group
=> The control group is 15% smaller than the IVM group (736 million vs 628 million). You would therefore expect fewer deaths in the control group. Yet there were in that group 7 times as much Covid deaths to regret.
Relative comparison: deaths per million inhabitants
The numbers can be 'popularized' in many ways.
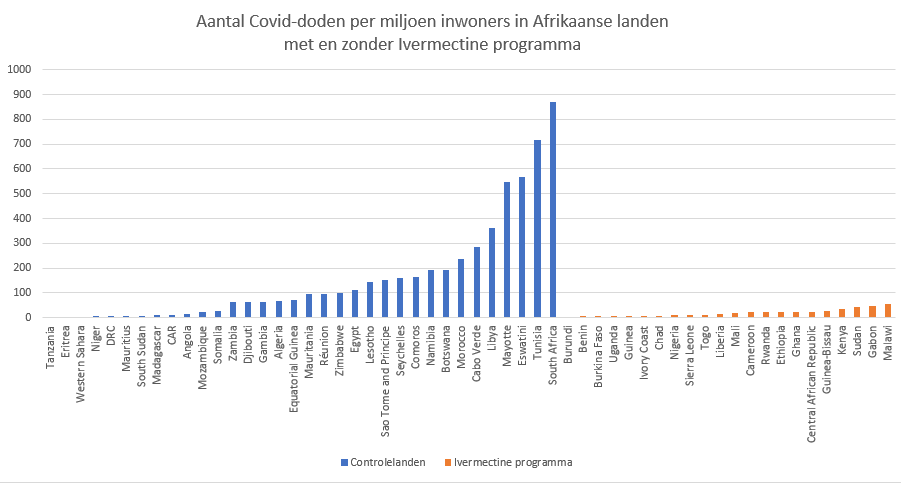
- The average of the IVM group is 20 deaths per million inhabitants.
- The average of the control group is 153 deaths per million inhabitants.
=> In African countries that do not have Ivermectin programs, mortality is on average more than seven times higher than in countries with Ivermectin programs.
- The highest mortality of Ivermectin countries is found in Senegal: 60 per million.
- In the control group, South Africa has the highest Covid mortality: 871 per million.
=> In countries without Ivermectin, Covid mortality is up to 14 times higher than in the worst-affected Ivermectin country.
Het "zwaarst getroffen" land zou een outlier kunnen zijn. Maar voor de top-3 geldt hetzelfde.
- The Top 3 IVM countries hardest hit by Covid have 60, 56 and 47 deaths per million inhabitants respectively. This amounts to a mortality of 0.006% of the entire population
- The Top 3 countries most affected by Covid in the control group have 871, 718 and 569 deaths per million inhabitants respectively. That is 0.084% of the total population.
=> The percentage of Covid deaths in the three worst-affected countries in the control group is 14 times higher than the three worst-hit IVM countries.
And you can continue like this:
- The top 20 states with the highest Covid deaths are all control group countries (there are even 22 of them).
- Most of those top-20 countries have more than twice as many deaths per million inhabitants as the worst Ivermectin country.
- The 35 countries with the lowest mortality include 100% of Ivermectin countries and less than half of non-Ivermectin countries.
Ivermectin (a 12 cents treatment) is simply not allowed! Basta!
How can there be a €150,000 fine for prescribing this medicine? Doctors are also climbing the scaffolding, read on the site of Medisch Contact in the comments what they think about that.
The trials that will conclusively prove that Ivermectin does help will certainly come. See references to some of the many preludes to this at the bottom of this article. Until then, we are dealing with a disastrous protocol approach. Models and statistics have been created to support us in what we observe and make predictions. Things are different now: what we observe is not true until we can artificially imitate it. We know that this is not actually a good verification of aerosols, it took decades before aerosols could be measured. And some still insist that didn't happen.
Would it help if you first had to prove that the 'apparent' Ivermectin effect in the graph is caused by something else?
Critical questions here:
- The countries where Ivermectin is used may be less urbanized and therefore less susceptible (? Upon inquiry it appears not to be the case, but I am not an Africa expert.)
- There are twelve countries without Ivermectin that also score below 60 deaths per million. That also requires an explanation, even if it is only 30% compared to 100%.
- De helft van de "Niet-Ivermectine"-sterfte komt uit Zuid-Afrika terwijl daar slechts 9% van de totale Afrikaanse bevolking woont. Daar moet toch wat over te zeggen zijn... (Maar goed: zelfs al laat je Zuid-Afrika buiten beschouwing, dan is er in de overige Ivermectinelanden nog steeds 7 keer zo weinig sterfte als in de "controlegroep".)
Scientific trends
De afweging om Ivermectine op deze manier te verbieden roept vraagtekens op. "... there is no scientific basis for Ivermectin's use to prevent or treat corona.", schrijft de Inspectie Gezondheidszorg en Jeugd. Dat ze dan geen andere oplossing of aanpak hebben is mij een raadsel. Maar dat zegt natuurlijk niks.
A very obvious explanation is that a well-functioning medicine would undermine willingness to vaccinate, but I don't want to think in such a conspiratorial way. The fact remains that a 'repurposed drug' costing 12 cents per treatment cannot expect the pharmaceutical push that a (much) more expensive patented vaccine to be rolled out worldwide does have. Because who wants to pay for a representative study for a disease that kills approximately 0.15% of the sick? That requires huge sample sizes and therefore deep, deep pockets. You will never earn that back from Ivermectin.
I also took a quick look at PubMed to see what studies there have been in recent months. I couldn't find any recent negative study:
We observed a preliminary beneficial effect on mortality associated with ivermectin use in patients with COVID-19, which warrants further clinical evidence in appropriately designed large-scale randomized controlled trials.
https://pubmed.ncbi.nlm.nih.gov/33779964/
hydroxychloroquine, lopinavir / ritonavir, ivermectin, artemisinine en nitazoxanide:
https://pubmed.ncbi.nlm.nih.gov/33776767/
Given how well the results of previous clinical trials for hydroxychloroquine and lopinavir/ritonavir are explained by the models presented here, similar strategies should be considered in future prioritization of drug candidates.
Monash University, Melbourne, Australia, led by Dr. Kylie Wagstaff, announced that an old and effective anti-parasite drug called ivermectin showed promise with early treatment, killing the virus within 48 hours. This drug was discovered in 1975 and marketed worldwide in 1981, showing significant efficacy in in vitro studies against influenza, HIV, Zika, and dengue viruses. One of the plus points of this drug is its price, which is about $0.12 for a full course of treatment.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7964257/
Ivermectin and remdesivir turned out to be the most promising drugs. Our results suggest that both drugs use different mechanisms at the entry and post-entry stages and can be considered as potential inhibitors of SARS-CoV-2 replication.
https://pubmed.ncbi.nlm.nih.gov/33746908/
SOC (Standard-of-care) treatment together with ivermectin did not lead to serious side effects. All patients showed a decrease in SARS-CoV-2 viral load within 7 days; however, those receiving ivermectin had a more consistent reduction compared to the SOC group alone, characterized by a shorter time to obtain two consecutive negative SARS-CoV-2 RT PCR tests.
https://www.sciencedirect.com/science/article/pii/S2214750021000445
Ivermectin is safe in patients with SARS-CoV-2, reducing the symptomatology and viral load of SARS-CoV-2. This antiviral effect appears to depend on the dose used, and if confirmed in future studies, suggests that ivermectin may be a useful adjunct to SOC treatment in patients with mild COVID-19 symptoms.
Favipiravir, ivermectin and interferons are approved in certain countries. Expert opinion: Global vaccination is now underway. Vaccines and antibodies are highly antigen specific and new variants are emerging. In addition to mass immunization, there is a need to treat outpatients who contract the disease. We call on public health authorities to allow treatments with known low risk and possible benefit to be used alongside mass immunization.
https://pubmed.ncbi.nlm.nih.gov/33721548/
https://c19ivermectin.com
https://ivmmeta.comwebsites with overviews of ivermectin studies
And so on, and so on... Get to work, doctors!
Objections that I received through various media I have dealt with in the post of 4 April
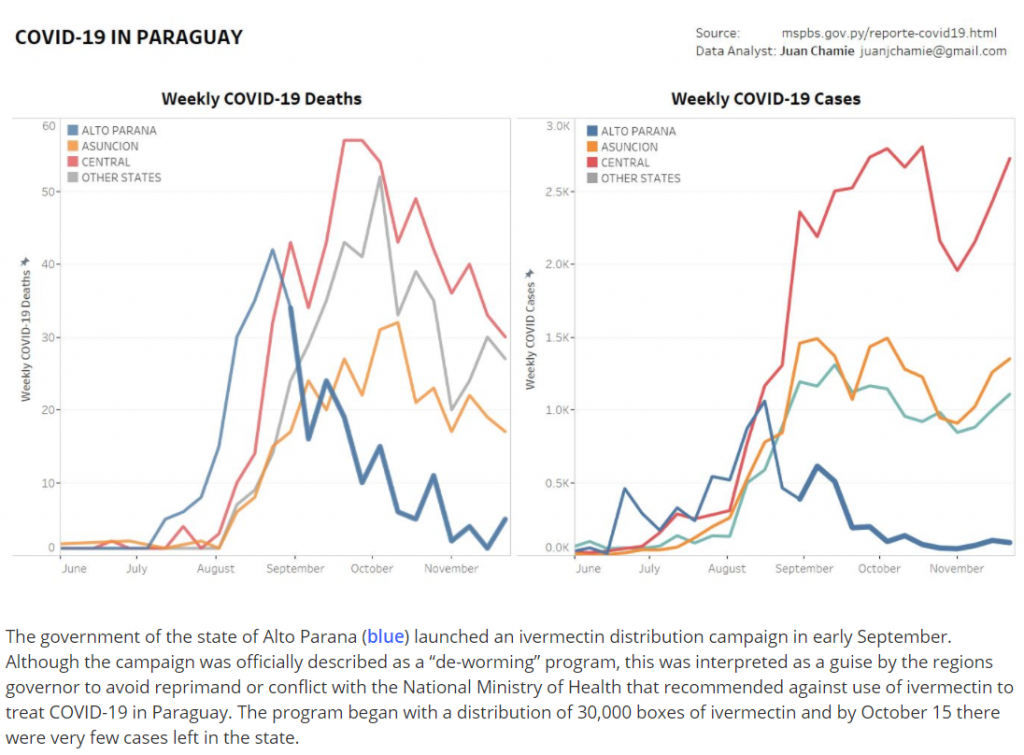
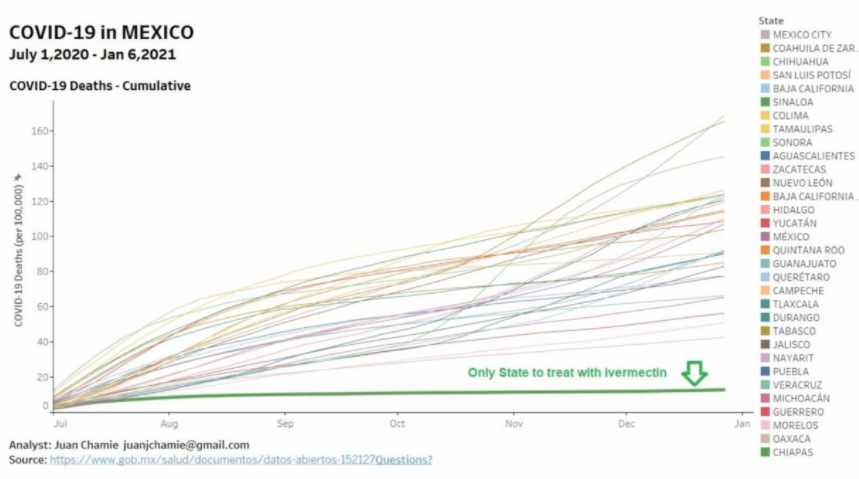
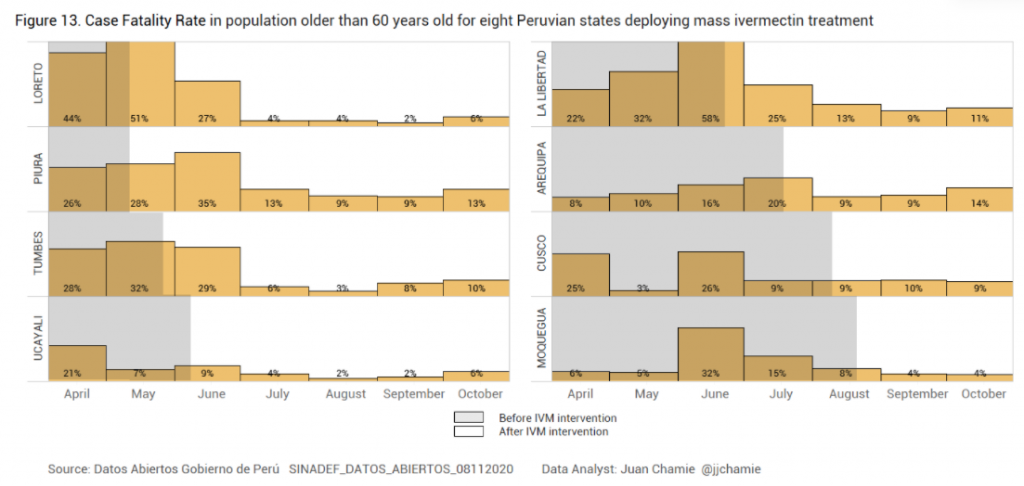
Some more examples from other parts of the world:
Objections that I received through various media I have dealt with in the post of 4 April
