
Bij het vorige artikel over een Deens onderzoek naar de variabele batchkwaliteiten, van eergisteren, had ik gisteren een kopje "Naschrift 3-7-2023" toegevoegd. Mocht je het artikel niet hebben gezien: het ging over een Deens onderzoek dat vreemde profielen in de vaccinbatches in Denemarken herkende. Verschillende sterftecijfers per batch samenvallend met verschillende prikhoeveelheden: van de meest dodelijke batches werden de minste prikken gezet en de minste dodelijke batches waren niet getest. In het artikel werd gevraagd om data waarmee dat te duiden zou zijn.
In the meantime, quite a lot of stuff has been made and I wanted to add that in that postscript afterwards. However, it became more and more extensive. See below.
Het Deense onderzoek (al anderhalf jaar oud!) is plotseling hot, vermoedelijk vanwege het interview met Duitse wetenschappers die het Deense onderzoek zorgelijk vinden en zijn gaan uitzoeken of ze iets soortgelijks in Duitsland waarnemen. Een van de Duitse wetenschappers die in de cijfers is gedoken liet zich tijdens het interview ontvallen: "Boze tongen zouden kunnen beweren dat placebo's er ook zo uitzien." Dat was een gedachte, een speculatie, maar absoluut niet de crux van het Deense artikel. En juist daar springt iedereen dan weer bovenop wat bijvoorbeeld leidde tot een artikel in The Daily Sceptic dat kopt "Pfizer Vaccine Batches in the EU Were Placebos, Say Scientists".
That is not what the Danish study is about. But that is what makes all kinds of people suddenly angry and look critically at that study.
What does the criticism boil down to
If we put aside the criticism of the spectacle headline about the suspected placebos - because the placebos are not stated anywhere else - there is still some criticism to be made about the study itself. This mainly concerns limitations that the Danes themselves also mentioned in their study. You can harp on that, but hey, we already knew that.
What several critics point to is the average age of the pricked, which could vary per batch color. Jessica Rose1 https://jessicar.substack.com/p/debunking-the-yellow-dot-lot-placebo found that the blue were on average 50 years old and the yellows 37 years old. She explains that the blue batches were set at the beginning of the year, hence the older population, which was first. That would explain the difference.
But 'average 50 years' would be something like 35-90 years and an average of 37 years: 15-45 or something like that. There is at least an overlap of about thirty/forty/fifty people in both groups, who should then have shown intermediate values between the blue and the other dots. That area is now virtually empty. So she did have a point, but not a very strong one in my opinion. I wrote that in a comment below her article and she liked it but did not comment further.
Haar argument strookt niet met wat een Duitse professor zegt in het interview met Preradovic: "These blue batches, from this dangerous batch, have appeared again and again and not only at the beginning or only in different countries, so widely distributed, both in time and geographically." Dat hadden ze nagekeken. Daar moet hij het dan maar eens met Jessica over hebben want dat klopt kennelijk niet.
Denis Rancourt2 https://denisrancourt.ca/entries.php?id=131&name=2023_07_01_does_the_analysis_of_schmeling_et_al_suggest_a_batch_dependent_safety_signal_for_the_bnt162b2_mrna_covid_19_vaccine vindt dat je met zulke beperkingen helemaal niet zulke stellige uitspraken mag doen. (Hij noemt zijn eigen schrijfstijl overigens "direct". Dan mag het kennelijk wel.) Maar de Denen doen helemaal geen stellige uitspraken. Zij wapperen hevig met een rode vlag en geven aan dat er zeer dringend data nodig zijn voor onafhankelijk vervolgonderzoek.
He actually makes the same age objection. He lists three reasons why missing age differences is crucial. He corresponded with the Danish authors about this and received the neat answer which showed that in all three groups the percentage of over-70s with side effects was similar and in the blue (most harmful line) even the lowest:
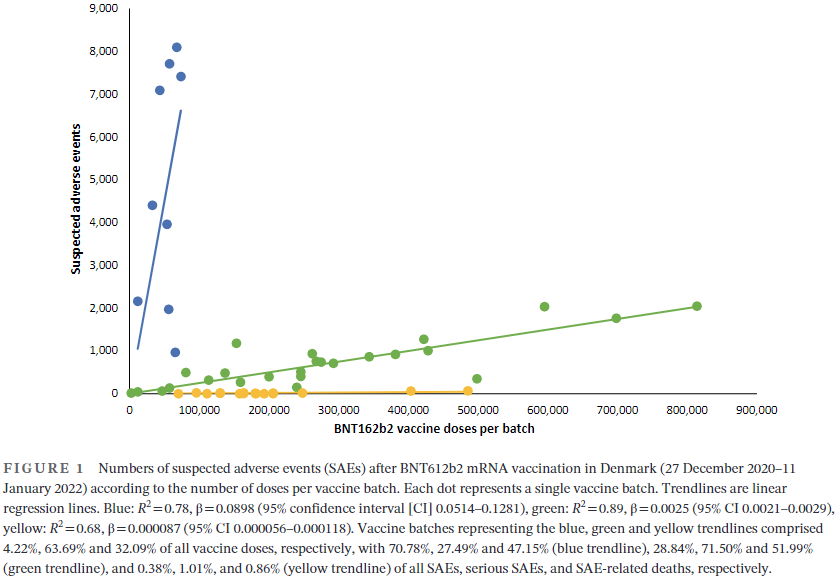
"The assumption that the age factor was responsible for the results may not be true. We now have access to data on the age of vaccinated individuals with reported SAEs, and in the high SAE batch group (blue trend line in Figure 1), only 21% of SAEs were reported in individuals aged 70 years or older, i.e. 79% were younger than 70 years (younger frontline healthcare workers were of course also among the first to be vaccinated). For the 'medium SAE batches' (green trend line), 22% were 70 years or older, and for the 'low SAE batches' (yellow trend line) this ratio was 27%. It therefore seems less likely that the selective administration to old and vulnerable individuals during the first phase of the pandemic was an important determinant of the 'emergence' of the high SAE batches."
In my opinion, this refutes the age confound as a determining factor for the distinction between the three vaccine profiles. Rancourt then continues to ramble on about what 'suggests' means and what exactly 'incorrect' is, but he firmly maintains his own point. I asked him in a comment why he did not accept those arguments, they seemed quite valid to me. He replied that I should read everything again. I did that dutifully, but it didn't help.
They're all males to me.
And then something else that struck me about Jessica Rose: there is a lot of belief that placebos cannot have any significant side effects. That is not correct and I have no idea where the threshold value is. Of course there are complaints after vaccinations, but are they more than normal? Does it really depend on the substance injected? That's exactly why you use control groups.
In any case, the placebo effect is very powerful, also in a negative sense (nocebo). People who are very afraid that they will get sick are often right. Even a sugar pill can make people vomit, as long as they are warned in advance that severe nausea is a possible side effect. (see also an earlier article on The Nocebo effect). An injection is a 'dramatic intervention', as Dr. Ben Goldacre calls that. A placebo injection has much more impact than a placebo pill. Even more than two pills. If 200,000 injections have been made without a single entry in VAERS, I would rather suspect a system error. Or most of those lots have been thrown away - but that is also speculation because we have no data, people are as silent as the grave.
Placebos don't have to be saline either. They can also have an almost identical composition to the real vaccine, but without the active substance (the mRNA). Anything can go wrong in the production of such a placebo.
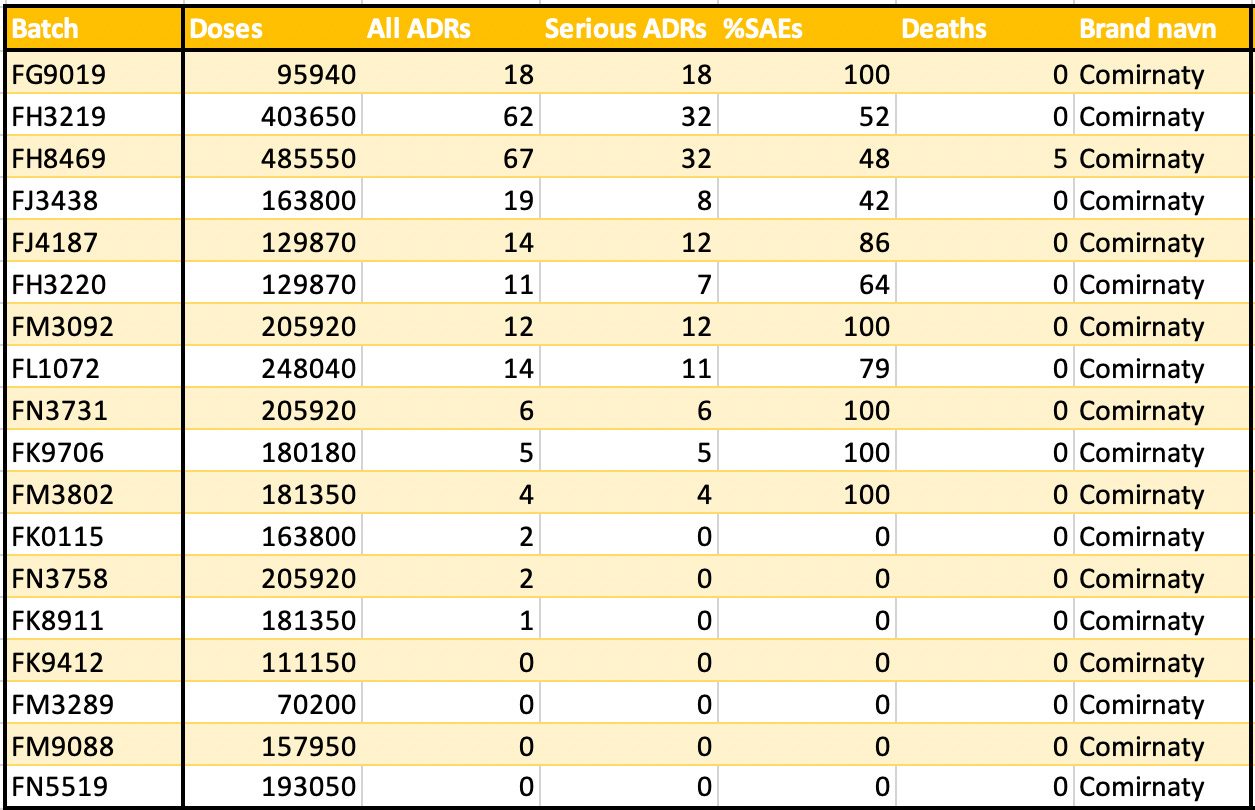
Jessica Rose shows a table of the 18 'yellow' lots. 0 (zero) deaths have been reported in 17 of them. The bottom four, together more than half a million jabs, have not produced any reports of side effects... The bottom seven, more than a million jabs: 4 side effects in total! Seems impossible to me.
The third from above, just under half a million jabs: 5 deaths! Strange, isn't it? That alone is a signal of possible product instability.
Spectacle speculation
The 'debunkers' sometimes speculate more than those they debunk to show how many other possibilities there are besides those suggested - which are not even included in the original research. So let me speculate for a moment.
If the blue batches were indeed set in the first months, the green batches in the summer and the yellow ones in autumn/winter, then you could also suggest that the increased natural immunity has had a protective effect against the vaccination side effects. The hypothesis is that if you have had Covid, your immune system has already had a training in clearing these spikes. That would immediately explain why Sweden has a lower post-vaccination excess mortality than other countries: the Swedes were already immune when vaccinations were carried out. The upside-down world: getting sick to protect you from vaccinations. I thought it was funny.
Without data, you can think of anything. No, Pfizer really does have something to explain.
(update July 6: Meanwhile, John Campbell has also picked up the Danish research.)
and this one preceded that (nothing new further)
Footnotes
- 1
- 2

Thanks for the update. I hadn't followed what Rose and Rancourt had published, but at least it's not an age confounder.
As far as I am concerned, placebos should only be inert substances. In other words, an injection that does not contain synthetic mRNA, but does contain toxic LNPs, and/or mercury, aluminum, etc. should not be called placebo, because it does contain active/toxic substances. Incidentally, pharmaceutical companies will try to get away with it to cover up negative side effects.
About your speculation at the end: Dr. Michael Palmer mentions that people with natural immunity react more violently because their immune system is trained and ready.
Reading tip: How to create a deadly pandemic in five easy steps
https://metatron.substack.com/p/how-to-create-a-deadly-pandemic-in
In March-April 2020, the amount of anti-inflammatory and coagulation inhibitors used (see also link below) decreased drastically. At exactly the same time there was a drastic increase in mortality.
https://bvnl.nl/corona/ooggetuigenverslag-van-een-bezorgde-arts-epidemioloog-tijdens-de-eerste-coronagolf/
The authorities said at the time that because of the unknown 'virus' we should not do anything until there was perfect scientific evidence.
This is how I can also create a 'pandemic': Write that because of the new virus people should not take in moisture. If there is excess mortality, you dedicate it entirely to the virus, and not to:
– fear (if you scare people to death, some will die from the stress)
– mass destruction measures (solitary confinement, also under a different heading such as isolation/quarantine, leads to increased mortality)
– iatrogenic treatments (remdesivir, early intubation, midazolam + morphine)
– absence of regular care (anti-inflammatory and coagulation drugs, dehydration)
– compensation for under-mortality from last flu season
– air pollution (Wuhan, Bergamo), dry air
Common in vaccine research is that during the discovery phase, the control group is given a composition with everything except the antigen (the substance against which an immune response is triggered).
There are also several articles about medication on this site, this one, for example.
The future will tell if Dr. Palmer is right. Vandenbossche constantly warned that the viruses would become increasingly dangerous, which is not so bad.
And these will also interest you, about the Nocebo effect
It is indeed common that the 'placebos' used are not inert placebos, but 'common' is not the same as 'good'.
The medicines authorities should never allow current practices. It should come as no surprise that they are doing it anyway, because in stark contrast to their public mandate, they are actually working for the pharmaceutical industry, not public health.
ICAN rightly fought (and won) in 2020 that inert placebos were enforced in the COVID vaccine trials. The pharma criminals did so reluctantly.
It is absolutely no coincidence that not only other 'vaccines' are used as placebos, but specifically the vaccines that are known to cause the worst side effects (such as 'against' rabies and meningitis). As a result, the side effects of the tested product appear to be less.
If you were to test the COVID poison shots against a cyanide 'placebo', they *seem* absurdly safe. (If the pharmaceutical companies were allowed to use a cyanide placebo, they were guaranteed to do so. Of course, they prefer not to do any research at all, because then they can continue to say that there is no conclusive evidence of negative side effects.)
I don't think anyone realizes that the placebos used are themselves toxic and that the pharmaceutical companies do this deliberately. The 'placebo' controlled trials only say something about the *relative* safety, not the *absolute* safety, when it should be about the latter.
I could still live with a placebo that causes some irritation, but is guaranteed to be safe. Maybe diluted vinegar? This way you have less chance of the placebo / nocebo effect, but serious side effects still come to light.
Incidentally, it is certain (to my knowledge) that the chance of side effects with the second COVID jab is much greater than with the first. (That in itself is good evidence of causation, see Bradford Hill criteria.) As far as I know, it is not known whether this is due to the mechanism that Dr. Palmer describes a different mechanism, but it ties in with what Palmer mentions.
Perfect timing: Dr. Vinay Prasad has just published the video below:
Placebo Control Arms | Vaccines – Which one? | Active vs Passive/ Inert Placebo | Standard of care |
https://www.youtube.com/watch?v=U4LuEPYMl_k
So what I said is indeed true. There are other irrational practices that need to be burned to the ground. I hope RFK will get something done. He should sit in Fauci's chair.
Did you see Ben Goldacre's hilarious Nerdstock performance about placebos in the articles? Let's see. Mandatory cost!
Would the secret agreements between pharmaceutical companies and governments say anything about this?
Perhaps it has been agreed that the active ingredient (or a different dose) will only be used in part of the batches, in order to be able to carry out a large-scale practical test.
An additional advantage is that due to a large number of placebos or a lower dose, any serious side effects are less noticeable.
In the meantime, there is a lot of money being made from it.
Or was there simply too little production capacity, and placebos were provided to meet obligations, and to give governments a means of reassuring the population? After all, vaccination was the solution to the pandemic...
Anton, take a quick look at this discussion by John Campbell with one of the authors of the Danish study........my pants fell off.
https://youtu.be/KgldG9r-i9M