
The first and probably not the last virus varia article in response to the "Final report on mortality and excess mortality 2020 and 2021" by CBS and RIVM. To be consulted via PDF and website.
A policy report of 82 pages... I would prefer to wait for the peer reviews that are always considered necessary in these circles, but I fear that they will never come. Of course, it is not a scientific publication either. However, there is a sounding board group to reflect critically.
Unfortunately, no accountant has been invited to that sounding board group, someone who wants to see the receipts for everything. Now the report gets stuck in assumptions, estimates, impressions, approximations. On what basis it is usually impossible to determine. They explain it willingly but show nothing. The hope was that, based on the same data, assumptions, estimates, impressions and approximations would also be made from a different perspective. An enforced monopoly on knowledge (and data => knowledge) is neither healthy nor credible.
The sounding board group thinks the same way, they indicate in their press release of 23 June:
PRESS RELEASE – June 23, 2022
OVER-MORTALITY RESEARCH CBS RAISES QUESTIONS
The research by Statistics Netherlands (CBS) into the causes of excess mortality up to and including November 2021 is too limited by access to medical data of deceased people. As a result, CBS's estimates of the ratio between excess mortality and Covid19 mortality are insufficiently substantiated. This is the opinion of members of the independent sounding board group that was set up by ZonMW, the organization for health research and care innovation, at the request of Minister Ernst Kuipers of Health, Welfare and Sport (VWS).
CBS conducted the study over the past four months on behalf of the Ministry of Health, Welfare and Sport in response to a motion by MP Pieter Omtzigt that was adopted by the House of Representatives on 1 December 2021.
The motion also led to the establishment of a sounding board group of independent experts who could provide advice and input on the results of the research. In a response to the final report, they advised CBS to indicate in the report what the shortcomings were in this study due to the limitations in access to data. The sounding board group found that there is 'quite a bit wrong with the data landscape and that it is not necessarily a lack of data, but a lack of access to data'.
According to the members of the sounding board group, the House of Representatives should be better informed about the problems surrounding data sharing. "There is a lot of discussion about exactly how many people have died from Covid-19 or from another condition. In addition, there is speculation about the effects of the Covid19 vaccinations and the delayed care on excess mortality," says health economist and sounding board member Eline van den Broek-Altenburg. "That is why it is important that there is clarity. Serious research is only possible if CBS, RIVM and science are given access to the necessary data."
The sounding board group also has doubts about the information in the cause-of-death certificates that CBS used to investigate excess mortality. The possible changes in coding and the way in which causes of death are recorded, such as in the electronic patient records of general practitioners and hospitals, can have an effect on the usability of the data and the research results. Ronald Meester, Professor of Probability Theory at VU Amsterdam and member of the sounding board group: "CBS is far too firm about the number of COVID-19 deaths. The inadequate registration, often based on no more than suspicions and symptoms, does not allow such a conclusion at all. In addition, not only primary causes of death must be considered, but also secondary and tertiary causes of death."
For information: https://www.zonmw.nl/nl/over-zonmw/coronavirus/onderzoek-naar-corona-en-covid-19/oversterfte/
Eline van den Broek – Altenburg
The motion has been ignored
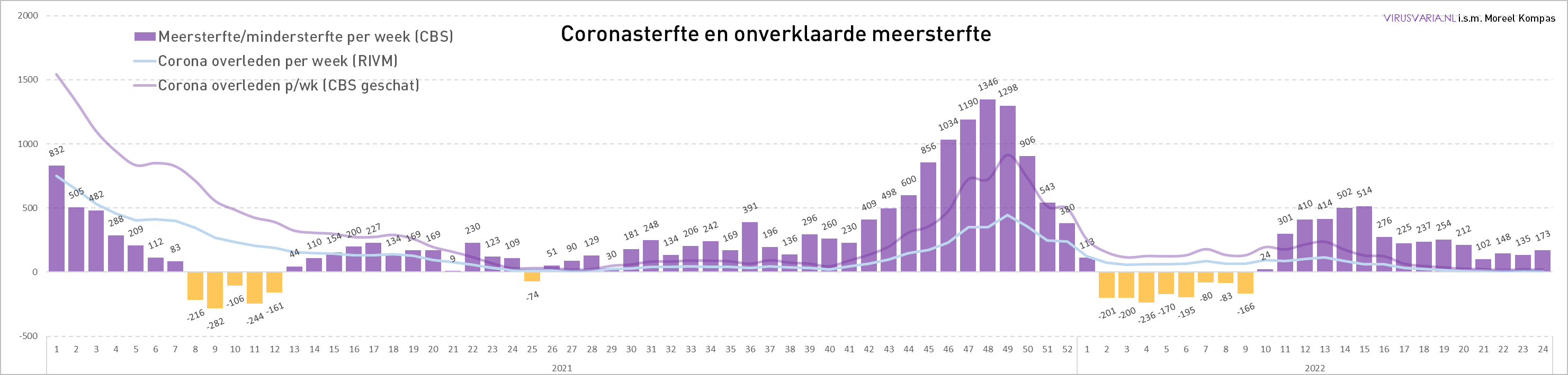
The Omtzigt motion, unanimously adopted on 1 December, speaks of "excess mortality in recent weeks" and "excess mortality up to and including November". In retrospect, that turns out to be an unfortunate restrictive formulation because we are now in June and the reporting period does indeed end in November, 7 months ago, while the following months are also interesting, especially Jan/Feb/Mar. Looking at the previous excess mortality, there is a very small undermortality in Jan/Feb and again excess mortality in March. ('Excess mortality' not to be confused with 'excess mortality'. Surplus mortality is the structurally sustained mortality above the expected level. So what is excess mortality? Excess mortality incidents are peaks that fall outside a fluctuation band, which is less relevant here.)
Last week, only 8% of the total 'excess mortality' was attributable to corona. The numbers are not high, but do we wait to figure it out until the water runs over the white nuggets again?
The motion for a specific explanation for this mortality level in that almost covid-free period was never carried out. According to CBS/RIVM, it was "the reason" to issue a policy report.
Furthermore, the motion asked for an "academic" investigation. Civil servants are sometimes academics, but that does not make it academic research. The external, independent academics involved (many of them Prof. Dr.) in the sounding board group were not given access to the underlying data of the explanation by CBS/RIVM as given in the report on the government's actions. It can be concluded from the minutes that they could only make editorial changes.
Actually, not a single aspect of the Omtzigt motion has been addressed. How such a specific question can give rise to such a broad smokescreen makes you think.
Some comments on the cbs/rivm policy report
Mortality expectation
Page 11: Explanation of how to determine mortality expectation: this is done on the basis of the years 2015-2019. One takes the averages, not the trend: "This average mortality per week provides an approximation of the expected weekly mortality. The trend in population ageing has not yet been taken into account. That is why the mortality per week has been rescaled to the expected total mortality for the year."
In summary: you choose a method that ignores trends (the average) and then correct what you suspect will have an influence: in this case, the trend of aging.
This approach easily leads to errors, interpretation bias and missing underlying trends. To demonstrate that, I put it in a graph.
If you extend the raw numerical trend (standard completion function in Excel), you have the gross figures including all trend developments and not just the known trends that make the decision to "rescale to the expected mortality for the year".
The expected mortality is therefore the average with an unclear rescaling correction. We do not know how this rescaling is calculated (presumably based on a model) but it is in any case about 1,000 below the "gross" trend. This leads to additional excess mortality rates that have to be corrected away. Maybe there is a wise choice behind it, maybe not. My confidence in the first possibility is negligible.
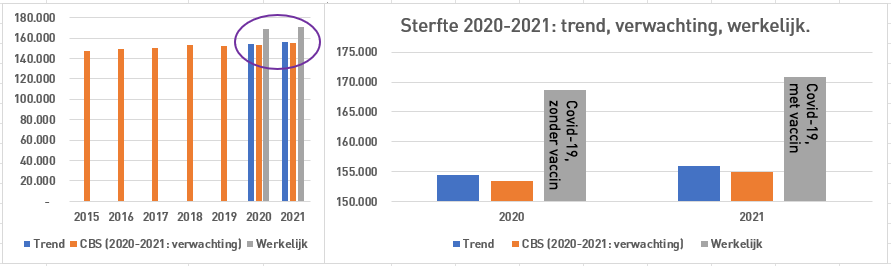
The grey bars show the mortality rates realised. Keep in mind that 2020 the covid-19 year without vaccination wax. According to the RIVM, Covid-19 was the biggest cause of death in 2020. 2021 was the year with vaccination and higher mortality.
On the designation as cause of death #1 was a bit of bargaining. For more ways to calculate excess mortality, I refer to an earlier article, which contains two links to reflections byBo van der Rhee on LinkedInand aartikel van Els Ooms, n.a.v. de cijfers van het Belgische RIVM “Sciensano”.
Het wordt maar weer eens bevestigd dat we naar het buitenland moeten voor zinvolle informatie. Wordt vervolgd.
0 reactions