
Steering on ICU capacity
The lockdown was intended to stay within the ICU capacity and that has been successful. The ICU people have had to work their butts off and are still doing so. On the radio it was reported that they even work 200% shifts – that may have been proverbial but it does give an impression. And they are not alone. We all stand behind them in solidarity: other patients are pushed back, wards are cleared, companies go under, unemployment rises, billions evaporate so that the ICU can do its job. They work very hard and it must be all the more frustrating to see that so many of their patients do not make it.

From the perspective of care, this is only logical. After all, the ICU is - among other things - also a last resort if nothing else helps and a patient feels that he can no longer breathe. Even if he can do so but his lungs no longer extract oxygen from the air, a doctor owes it to his task and his position to get the most out of every patient. Even in almost hopeless situations, a doctor must be able to persevere, even to the point of hopeless treatments in the ICU. That is admirable and at the same time you should protect doctors from themselves. They could undoubtedly do more for more patients.
For a few weeks now, we have been seeing more or less what that overcrowded ICU has meant so far. Thanks to the ICU, the mortality rate from corona has been reduced by one-tenth of a percent: 0.1%. That means: 1 in 1000 corona-infected people has been saved by the ICU. The RIVM does not have exact figures - we are used to that by now - but according to them it is something like 1.4% instead of 1.5% mortality among corona patients, around and near. Or 1.1% instead of 1.2%. So that is an effect. Can we also look at how that effect relates to the efforts? It's almost sacrilege, but I'll take the risk anyway.
The success rate of ICU treatment in numbers
The mortality rate of corona patients in the ICU is sometimes estimated at 20%. Unfortunately, for corona patients, this fluctuates between 65%-70%. So the survival rate is about 1 in 3.
In Italy, the results were even worse. There they also admitted patients with no chance than in the Netherlands. The horror images we have seen could have been prevented if an age limit (and/or later: a BMI limit) had been used. If Italy had used stricter guidelines, promising patients who have now died in the corridor would still have had a chance. In Italy it was more of a glorified hospice. They didn't have the capacity for that.
The Netherlands, April 22
[28-4: numbers are higher, key point still valid]
In the past 6 weeks, 2680 ICU patients have been admitted [28-4: 2773]. Of these, 965 were still in the ICU on 22 April [28-4: 788]. Of the remaining 1715 ex-ICU patients [28-4: 1985], 572 [28-4: 625] came out of the ICU alive* (indeed: 33%). The data comes from the Dutch Intensive Care Evaluation Foundation. It is not known how many of these patients die later.
The blue line indicates that fewer people leave the hospital alive than come out of the ICU alive. But the delay also plays a role here and we also do not know how long ICU patients stay in hospital on average. So because of (again) the incompleteness of the data, we leave this out of consideration.

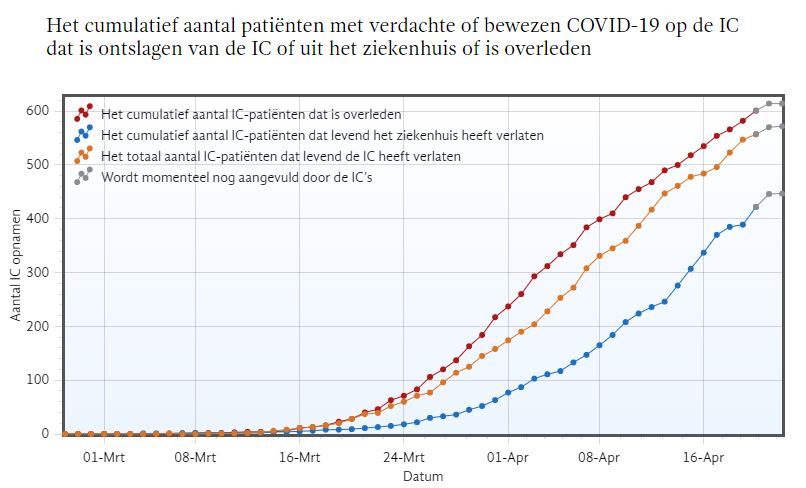
Source (dated 22 April): National Intensive Care Evaluation
There are about 550,000 people infected with the virus. (source dated April 16: Sanquin Hotels) Hence, the 572 ICU patients rescued represent 0.1% of mortality among infected people. The assumption is that the ICU survivors would not have made it without ICU, so that, for example, (home) treatment with medication and oxygen would not have helped.
I will leave aside the possibility that the ventilator has worsened the condition of many patients. There are indications of that, but that is all there is to it at the moment.
Conclusion
As a non-physician and non-economist, I would like to hear that the treatment contributes to public health and is affordable in accordance with the current standards or perhaps 2x the current standards. My main reason for writing this piece is that considerations such as these seem to be ignored.
This relativization may read like a direct attack on everything that has to do with IC. This is emphatically not the intention. What is intended: the policy focus on the ICU and what is thrown into the fight for it requires an ongoing evaluation of our targets, our performance and the ROI in terms of public health and well-being. I have not yet seen any trace of an evaluation.
An even sharper thought experiment: suppose a pharmaceutical company would come up with a corona drug, 'FiniCor'...
NEW! FINICOR!
The cure that has been proven to put an end to all your corona complaints!
- Is no corona treatment working? Then you are automatically eligible for the Finicor cure!
- FiniCor is only provided to patients who continue to deteriorate in the hospital despite medical care. Finicor has been proven effective in 33% of these patients. Those for whom the drug does not work (about two-thirds) will unfortunately still die.
- The cure lasts about 3 weeks. After treatment with FiniCor, an intensive rehabilitation period is desired. This can sometimes last up to 2 years.
- The production capacity for FiniCor is limited. In order to meet demand, the country will have to go into lockdown. This limits the rate of immunization so that supplies can be spread over a longer period of time.
Would this drug come on the market?
Money is not just 'money'. It also stands for culture and care.
Then also a financial consideration: the billions that are being invested now will later mainly be at the expense of public services such as culture and health care. Health care is perhaps the most important of these (I say as a music maker).Shortages in healthcare budgets will be at the expense of public health. I myself have Not the expertise to calculate how every billion less translates into disease and death. 'Poverty kills', the figures show that, but that's all I know. However, the scenario in which the healthcare system itself has to be put on a ventilator is not so difficult to imagine.
So I would like to see a discussion about when we are going to make difficult decisions, now or in the future when the money runs out? At the moment we still have options, but then, after the crisis, we are faced with a fait accompli that may cost many more lives than we have saved. Then we have 'Regret afterwards for what we have now left behind', to speak with Rutte.
*Living from the ICU: In addition, a minority of survivors are back on their feet after a few months. The majority are not in good shape with permanent lung damage and/or psychological trauma. No one is surprised by a two-year rehabilitation. By no means all ex-ICU patients can resume their former lives afterwards.