
shortlink: https://t.ly/gbaa
Aseem Malhotra, een controversiële cardioloog, gevaccineerd, overtuigde zijn patiënten om zich vooral tegen Covid te laten inenten. Hij ondersteunde het ‘narratief’ volledig, totdat zijn vader onverwacht en onverklaarbaar overlijdt. Het bleek een hartstilstand na pijn op de borst. En dat terwijl hij zijn vader nog vrij recent had onderzocht. De zoektocht die daarop volgt beschrijft hij in een Case Study, vandaag gepubliceerd. Omdat het zo’n toegankelijk en goed onderbouwd (peer reviewed) verhaal is deel ik het hier in het Nederlands. Ik realiseer me ook dat het hier alleen over hartproblematiek gaat. Ik heb het vermoeden dat we soortgelijke verhalen ook nog op andere vakgebieden gaan zien: herseninfarcten, oplaaiende kanker, neurologische problemen… Het blijft vooralsnog gissen.
Steve Kirsch's interview with Paul Marik, a well-known name for concerned coronavirus vaccine critics, was also published yesterday. Carried on his hands and remarkably often quoted doctor – until he sounded the alarm about the vaccines. He says in that interview, among other things:
"Covid revealed the corruption that was there for a long time. I had to unlearn everything I had learned. I relied on RCTs and they turned out to be perverted and corrupted by Big Pharma."
Dr. Paul Marik during his interview on Steve Kirsch's podcast
Strong language. Your career will be based on it. Marik says that it took a while before he could accept how the reality around the corona vaccines worked.
I find it extraordinary that Aseem Malhotra is not one of the usual suspects who, as a doctor, questions the "safe and effective" narrative. He is also still a doctor, his license has not yet been taken away from him (listen to the interview with Marik if you want to hear how that works).
[edit: I just saw that Robert Malone has one substack has dedicated to, with a video of Malhotra in it.]
Below is the translation of the two articles from The Journal of Insulin Resistance. The 48 references refer to the original english article. There you will also find the document and research details, PDF/XMS/EPUB versions, contact addresses etc. If you read English well, please go there. This is Part 1 only. For Part 2 of the paper look here.
Fighting the COVID-19 mRNA vaccine misinformation pandemic with true evidence-based medicine – Part 1
Vaccines save lives
The development of safe and highly effective vaccines in the second half of the 20th century is one of the greatest achievements of medicine. The prominent scars on my left arm are a constant reminder of the success of our ability to contain some of the deadliest diseases like smallpox, tuberculosis (TB), measles, mumps and rubella, to name a few. It is estimated that the traditional vaccines together save about 4 to 5 million lives per year1. The greatest success of vaccination was the global eradication of smallpox, which had a mortality rate of 30%.2
In other words, nearly one in three people who contracted smallpox died. The development of a safe and effective vaccine after much trial and error led to 95 out of 100 people being protected from symptomatic smallpox infection and immunity lasting five years, completely eradicating the virus in the seventies. Similarly, one dose of measles vaccine is said to be "95% effective." What is meant by that? Most people assume that 95 out of 100 people who get the inoculation are protected from symptomatic infection and transmission and also have long-term immunity. Similarly, when exposed to chickenpox, only five out of 100 vaccinated children will contract this disease.
Vaccines are also among the safest interventions in the world compared to most drugs used in the treatment of chronic diseases, as we should expect, since they are administered to prevent something in healthy people and not to treat a disease. Therefore, it was good news that in the summer of 2020, several pharmaceutical companies, including Pfizer and Moderna, announced the results of their two-month randomized controlled trial, which showed that they had developed a vaccine with an effectiveness of more than 95% to prevent infection of what was at the time the most circulating strain of the coronavirus 2019 (COVID-19).
The experience of a doctor
Als vrijwilliger in een vaccinatiecentrum was ik een van de eersten die eind januari 2021 twee doses van het mRNA-vaccin van Pfizer kreeg. Hoewel ik wist dat mijn individuele risico klein was van COVID-19 op 43-jarige leeftijd met optimale metabolische gezondheid1, was de belangrijkste reden dat ik de prik nam om overdracht van het virus aan mijn kwetsbare patiënten te voorkomen. Begin 2021 werd ik zowel verrast als bezorgd door een aantal van mijn vaccin-weigerachtige patiënten en mensen in mijn sociale netwerk die mij vroegen om commentaar op wat ik op dat moment beschouwde als louter “anti-vax” propaganda.
I was asked for Good Morning Britain after a film director, Gurinder Chadha, Order of the British Empire (OBE), who was previously wary of vaccines and was also interviewed, explained that I had convinced her to take the jab.
Maar een paar maanden later gebeurde er een zeer onverwachte en uiterst schrijnende persoonlijke tragedie die het begin zou zijn van mijn eigen reis naar wat uiteindelijk een openbaring en eye-opening zou blijken te zijn, zo diepgaand dat ik na zes maanden van kritische beoordeling van de gegevens zelf, en gesproken hebbend met vooraanstaande wetenschappers die betrokken zijn bij COVID-19 onderzoek, de veiligheid en ontwikkeling van vaccins, en met twee onderzoeksjournalisten, langzaam en met tegenzin heb geconcludeerd dat, in tegenstelling tot mijn eigen aanvankelijke dogmatische overtuigingen, het mRNA-vaccin van Pfizer lang niet zo veilig en effectief is als we aanvankelijk dachten. Deze kritische beoordeling is gebaseerd op het analytische kader voor het beoefenen en onderwijzen van evidence-based medicine, waarbij specifiek gebruik wordt gemaakt van individuele klinische expertise en/of ervaring met gebruikmaking van het beste beschikbare bewijsmateriaal en rekening wordt gehouden met de voorkeuren en waarden van de patiënt.
A case study
Case studies are a useful way to convey complex clinical information and can reveal useful data that would be lost or not made clear in the summary results of a clinical trial.
On July 26, 2021, my father, Dr Kailash Chand OBE, former deputy chairman of the British Medical Association (BMA) and its honorary vice-chairman (who had also taken both doses of the Pfizer mRNA vaccine six months earlier) went into cardiac arrest at home after chest pain. A later investigation found that a significant delay in the ambulance likely contributed to his death.3 But I found his post-mortem findings particularly shocking and inexplicable. Two of his three major arteries had severe blockages: 90% blockage in his left vein and 75% blockage in his right heart vein. Considering he was an extremely fit and active 73-year-old man, who had walked an average of 10-15000 steps a day during his entire lockdown, this was a shock to everyone who knew him, but especially to me. I knew his medical history and lifestyle in detail. My father, who had been an avid athlete all his life, was fitter than the vast majority of men his age. Since the previous heart scans (a few years earlier, which had revealed no significant problems with perfect blood flow through his arteries and only slight ramps) he had stopped sugar, lost belly fat, reduced the dose of his blood pressure pills, had started regular meditation, reversed his prediabetes and even massively lowered his triglycerides in the blood, which significantly improved his cholesterol profile.
I couldn't explain his postmortem findings, especially since there was no evidence of a real heart attack but with severe blockages. This was exactly my own special area of research. That is, how to slow and even reverse the progression of heart disease. In my own clinic, I successfully prescribe a lifestyle protocol to my patients based on the best available evidence on how to achieve it. In fact, I co-authored a highly impactful peer-reviewed paper with two internationally renowned cardiologists (both editors of medical journals) on shifting the paradigm on how heart disease can be most effectively prevented through lifestyle changes.4 We benadrukten het feit dat coronaire hartziekte een chronische inflammatoire aandoening is die wordt verergerd door insulineresistentie. In november 2021 werd ik geattendeerd op een peer-reviewed abstract gepubliceerd in Circulation, met verontrustende bevindingen. Bij meer dan 500 patiënten van middelbare leeftijd onder regelmatige follow-up, met behulp van een voorspellend scoremodel gebaseerd op ontstekingsmarkers die sterk gecorreleerd zijn met het risico van een hartaanval, werd het mRNA-vaccin in verband gebracht met een significante verhoging van het risico van een coronaire gebeurtenis binnen vijf jaar van 11% vóór het mRNA-vaccin tot 25% 2-10 weken na het mRNA-vaccin. Een vroege en relevante kritiek op de geldigheid van de bevindingen was dat er geen controlegroep was, maar toch, zelfs als het gedeeltelijk juist was, zou dat betekenen dat er een grote versnelling zou zijn in de progressie van coronaire hartziekte, en belangrijker nog, het risico van een hartaanval, binnen enkele maanden na het nemen van het vaccin. Ik vroeg me af of de Pfizer-vaccinatie van mijn vader, die hij zes maanden eerder had gekregen, kon hebben bijgedragen tot zijn onverklaarbare vroegtijdige dood en dus begon ik de gegevens kritisch te beoordelen.
Doubts about the data
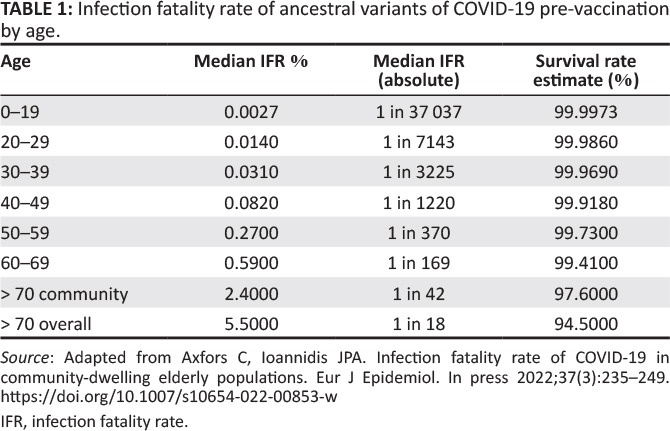
I remember a fellow cardiologist informing me, to my surprise at the time, that he had decided not to take the vaccine for a number of reasons, including his personal low background risk of COVID-19 (see Table 1)6 and concerns about unknown short- and longer-term damage. One thing that troubled him about Pfizer's crucial mRNA study, published in The New England Journal of Medicine, was the data in the supplement, specifically that there were four cardiac arrests in those who took the vaccine, versus only one in the placebo group. 7
These figures were small in absolute terms and did not achieve statistical significance in the study, suggesting that it may just be a coincidence, but without further studies it was not possible to rule out that this is a true causal relationship (especially without access to the raw data), in which case it could cause a wave of cardiac arrests once the vaccine is distributed to tens of millions of people around the world.
In terms of effectiveness, headlines around the world made very bold claims of 95% effectiveness, with the interchangeable use of "effectiveness" and "effectiveness" obscuring the stark difference between controlled trials and real-world conditions.8 It would be understandable to the lay public and doctors to interpret this as meaning that 95% of people would be protected from infection if 100 people were vaccinated. Even the director of the Centers of Disease Control (CDC), Rochelle Walensky, recently admitted in an interview that it was the first reports from CNN that made her optimistic that the vaccine would significantly stop transmission and infection, but it later turned out that this was far from true for the COVID-19 vaccines.9 The original trial found that a person was 95% less likely to contract the fall variant of COVID-19. This is known in medical terms as relative risk reduction, but in order to know the true value of a treatment, one must consider for that person how much their individual risk has been reduced by the intervention – i.e. the absolute individual risk reduction.10
Importantly, the trial results indicate that the vaccine only prevents someone from getting a positive test with symptoms, and that the absolute risk reduction for that is 0.84% (0.88% reduced to 0.04%). In other words, if 10,000 people had been vaccinated and 10,000 had not, for every 10,000 vaccinated people in trial, 4 people would have tested positive with symptoms, compared to 88 who had not been vaccinated. Even in the unvaccinated group, 9,912 out of 10,000 (more than 99%) would not have tested positive during the trial period. Another way to express this is that you would have to vaccinate 119 people to prevent one such symptomatic positive test (which is supposed to indicate an infection, which in itself is potentially misleading, but beyond the scope of this article).
This absolute risk reduction (0.84%) is extremely important for doctors and patients to know, but how many of them were told this when they got the jab? Transparent communication about risks and benefits of each intervention is a core principle of ethical, evidence-based medical practice and informed consent.11
The Academy of Medical Royal Colleges made this clear in an article published in the BMJ in 2015.12A co-author at the time was also the then president of the General Medical Council. Gerd Gigerenzer, the director of the Max Planck Institute, even stated in a 2009 World Health Organization (WHO) bulletin: "It is an ethical imperative that every doctor and patient understands the difference between relative and absolute risks to protect patients from unnecessary fear and manipulation."13
Contrary to popular belief, the study did not show a statistically significant reduction in serious illness or COVID-19 mortality from the vaccine during the six months of the study, but the actual number of deaths (attributed to COVID-19) is still important to note. There were only two deaths from COVID-19 in the placebo group and one death from COVID-19 in the vaccine group. Looking at all-cause mortality over a longer period of time, there were actually slightly more deaths14in the vaccine group (19 deaths) than in the placebo group (17 deaths). Also noteworthy was the extremely low number of cases of COVID-19 disease identified as severe in the placebo group (nine severe cases out of 21,686 subjects, 0.04%), indicating a very low risk of serious illness, even in areas chosen for the study because the infection was thought to be common.
Finally, the trials in children did not even show a reduction in symptomatic infections, but used the surrogate measure of blood antibody levels to establish efficacy, although the link between the antibody levels caused by the Wuhan spike vaccine and protection against infection is weak at best. The Food and Drug Administration (FDA) website states that:
The results of the currently permitted SARS-COV-2 antibody tests should not be used to evaluate a person's level of immunity or protection against COVID-19 at any time, and certainly not after the person has received a COVID-19 vaccination.15
Now that we know what the published trial did and did not show in terms of vaccine efficacy, we can try to extrapolate what the effect of the vaccine would be in reducing the mortality rate or other negative consequences of the virus. If there is a 1 in 119 chance that the vaccine will protect you from symptomatic infection by ancestral variants, then in order to find protection against mortality, this figure (11 = 119), must be multiplied by the number of infections leading to one death for each age group. This would result (up to two months after the vaccination) in the absolute risk reduction (before death) of the vaccine. For example, if my risk of dying from Delta at age 44 (should I become infected with it) is 1 in 3,000, then the absolute risk reduction of the vaccine that protects me from death is 1 in 3,000 multiplied by 119, so 1 in 357,000.
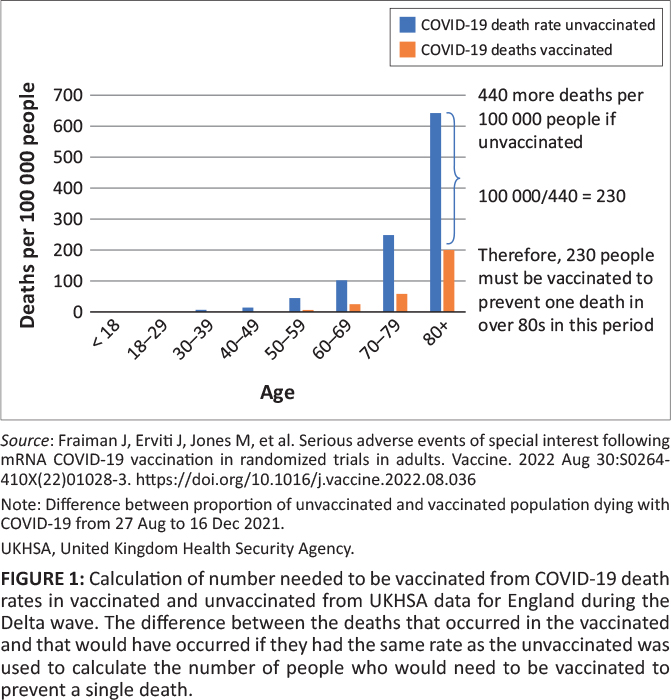
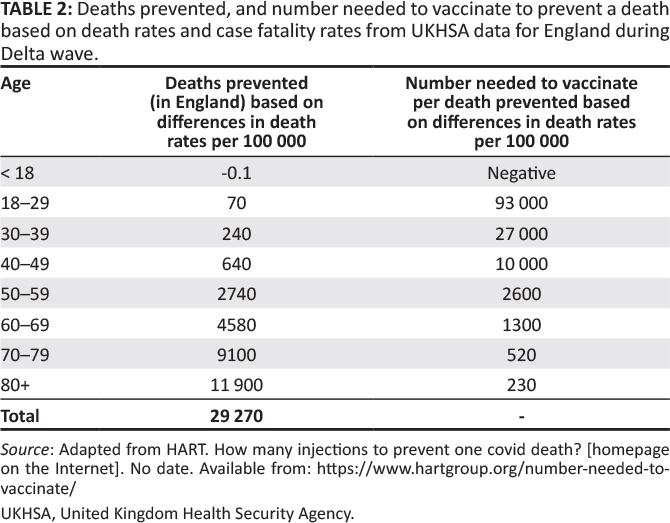
Of course, even for the people who become infected, the vaccination can provide some protection against death. Observational data can be used to calculate how many people need to be vaccinated to prevent a COVID-19 death. A comparison of population mortality rates16 for example, during the Delta wave indicates that 230 over-80s need to be vaccinated to prevent one death during that period, while that number rises to 520 for 70-year-olds and 10000 for 40-year-olds (see Table 2 and Figure 1 17).
However, these figures are distorted by inaccuracies in the measurement of the size of the unvaccinated population. As also noted in a recent editorial by John Ioannidis in BMJ evidence-based medicine, the vaccine's efficacy derived from non-randomized trials may be "spurious," with the bias caused by "pre-existing immunity, misclassification of vaccination, differences in exposure, testing, confusion due to disease risk factors, hospitalization decisions, differences in treatment use, and attribution of death".18
These figures refer to the entire population of England and do not necessarily apply to the healthy population; More than 95% of the deaths involved people with pre-existing conditions.19 It is also important to note that the vaccinated and unvaccinated populations differ from each other in other ways, which can skew mortality rates. For example, the unvaccinated are more likely to belong to a lower socioeconomic population, putting them at greater risk of serious illness or death if infected.
Professor Carl Heneghan, the director of the Centre of Evidence Based Medicine at Oxford, has explained his own clinical experience with the bias of healthy users. Some of his own patients who ended up in intensive care unit (ICU) with COVID-19 (classified as unvaccinated) did not take the vaccine because they were already suffering from a terminal illness.
Given these limitations, the above figures are likely to be an overestimation of the individual benefit of vaccination; Discussing such uncertainties openly and honestly is an essential part of shared decision-making.
What should be part of the discussion about shared informed consent when someone is considering taking the jab is something along these lines: Depending on your age, hundreds or thousands of people like you should be injected to prevent one person from dying from the Delta variant of COVID-19 over a period of about three months. For people over 80, this number is at least 230, but it rises the younger one is, to at least 2,600 for people aged 30 and over, 10,000 for people aged 40 and 93,000 for people aged 18 to 29. For omicron, which has been shown to be 30%-50% less lethal, that means significantly more people need to be vaccinated to prevent one death. How long the protection actually lasts is unknown; Currently, in some countries, boosters are recommended after only 4 months.
But how many people have had a conversation even close to such a statement? Not to mention the known, unknown and not yet fully quantified damage.
While many have proposed that omikron is intrinsically less lethal (supported by the observed molecular differences between omikron and the Wuhan-type virus), the immunity built up from previous exposure to protect against severe disease is also likely to be relevant to some extent. The crucial point is that, whether viral or immune-related, the milder nature of omikron is evident in the unvaccinated and therefore the reduction in mortality should not be attributed to vaccines.
What are the disadvantages?
Concerns have already been raised about the underreporting of adverse events in the clinical trials for the COVID-19 vaccines. Investigating medical reporter Maryanne Demasi analyzed the various ways the pivotal mRNA tests failed to account for serious damage.20 Not only were trial participants limited to the types of side effects they could report on their digital apps, but some participants who were hospitalized after the inoculation were taken out of the trial and not reported in the final results. After two months in the pivotal trials, the FDA allowed vaccine companies to offer the vaccine to subjects in the placebo group, essentially torpedoing any chance of proper record of side effects from then on and forcing a reliance on pharmacovigilance data.
Such data shows that one of the most common damage caused by the mRNA COVID-19 vaccine is myocarditis. A study in several Scandinavian countries showed an increased risk of mRNA vaccination relative to background, especially in young men.21 Authorities have repeatedly claimed that myocarditis is more common after COVID-19 infection than after vaccination.22 However, research data showing that vaccination reduces the risk of myocarditis in later infection is elusive, and in fact, the risks may be additive. The incidence of myocarditis skyrocketed from spring 2021, when the vaccines were rolled out to the younger cohorts who had remained within normal levels throughout the year before, despite COVID-19,23with the most recent evidence, a paper from Israel24found that the infection itself, prior to the vaccine rollout, did not increase the risk of myocarditis or pericarditis from COVID-19, strongly suggesting that the increases observed in previous studies were due to the mRNA vaccines, with or without COVID-19 infections as an additional risk in the vaccinated.24
Indeed, this reflects my own clinical experience advising and guiding several patients in the community who presented with a clear suggestion from the history of myocarditis after mRNA vaccination, but who were not necessarily unwell to be hospitalized. A very fit lady in her 50s developed fatigue and shortness of breath with exercise a few weeks after her second Pfizer injection. An echocardiogram showed severe impairment of her left ventricular function. Another 30-year-old lady developed similar symptoms with disturbing palpitations within a few days of her second injection; an ultrasound also showed a slight deterioration in left ventricle function, and a subsequent MRI scan of the heart showed several areas of lategadolinium elevation, a feature seen on the scan that corresponds to damaged heart tissue, and since heart cells cannot be replaced, this is likely to have long-term consequences.
Although vaccination-induced myocarditis is not often fatal in young adults, MRI scans show that about 80% of those who are hospitalized have some degree of myocardial damage.25,26It is as if one gets a small heart attack and suffers a – probably permanent – injury to the heart muscle. It is uncertain how this will play out in the longer term, including whether and to what extent this will increase the risk of poor quality of life or possibly more serious cardiac arrhythmias in the future.
A number of reports, depending on age, have yielded rates of myocarditis ranging from 1 in 6,000 in Israel27 up to 1 in 2,700 in a study in Hong Kong involving male children and adolescents aged 12-17.28Most epidemiological studies that have been conducted have measured cases of myocarditis diagnosed in a hospital setting, and do not pretend to be a complete measurement of more mild cases (from which long-term damage cannot be excluded). Moreover, underreporting of adverse events is the scourge of pharmacovigilance data.29
The UK relies on the Medicines and Health Regulatory Agency's (MHRAs) "Yellow Card" reporting system,30 which is far from sufficient for a rapid rollout of a brand new product. It discovered the clotting problems that led to the withdrawal of the AstraZeneca product in April 2021 for young people only after 9.7 million doses had been administered in the United Kingdom31; in Denmark, on the other hand, the problem was discovered after only 150,000 doses were administered.32
In the United Kingdom, almost 500,000 reports of adverse events have been registered since the distribution of the vaccine (via the yellow card system) in relation to the mRNA COVID-19 vaccinations, involving more than 150,000 people. In terms of the number of reports per person (i.e. who has received at least one dose), the MHRA's figures show that around 1 in 120 people have a probable adverse event that is more than minor.30However, the MHRA is not clear about the percentage and does not distinguish between serious adverse events. Nevertheless, this level of reporting is unprecedented in the modern medical era and equal to the total number of reports received in the first 40 years of the yellow card notification system (for all medicines – not just vaccines) until 2020.33 By comparison, for the measles, mumps and rubella (MMR) vaccine, the number of reports per vaccinated person was about 1 in 4,000, more than thirty times less often than the 1 in 120 reports of the yellow card for recipients of a COVID-19 vaccine.34 Norway does separate the reported serious side effects and shows a rate of about 1 in 1000 after two doses of BioNTech/Pfizer mRNA product that lead to hospitalization or are life-changing.35
Another, more useful source of information (due to the level of detail of each report made available to the public) is the United States (US) Vaccine Adverse Effect Reporting System (V AERS). As with the UK's system, the number of reports – including serious ones – associated with COVID-19 vaccines is completely unprecedented. For example, as of March 02, 2022, more than 24,000 deaths have been recorded in VAERS; 29% of them occurred within 48 hours of the injection and half within two weeks. The average reporting rate before 2020 was less than 300 deaths per year. An often given explanation for this is that the rollout of the COVID-19 vaccine is unprecedentedly large; however, this does not hold true since the United States has administered 150 million -200 million vaccinations annually (at least for the past decade). Another criticism of V AERS is that "anyone can make a report", but an analysis of a sample of 250 premature deaths found that the vast majority are reports by hospitals or doctors36Knowingly filing a false VAERS report is a violation of federal law that is punishable by a fine and imprisonment.37
Since VAERS was set up to generate early signals of potential harm for new vaccines, and has played a role in the process for several products, it seems perverse to criticize it as unreliable only now, when no changes seem to have been made to its operation.
It is estimated that the serious adverse events that are officially reported are in fact a gross underestimate, and this should be kept in mind with the above comments on VAERS reports. For example, an article by David Kessler (former FDA commissioner) cites data showing that only 1% of serious adverse events are reported to the FDA.38Similarly, in relation to the yellow card scheme in the United Kingdom, it is estimated that only 10% of serious adverse reactions are reported.39,40 A recent pre-publication co-authored by some of the most trusted medical scientists in the world in connection with data transparency adds validity to pharmacovigilance data. By consulting data from the FDA and Health Canada websites and combining results from journal articles publishing the Pfizer and Moderna trials, the authors concluded that the absolute risk of a serious adverse event from the mRNA vaccines (a rate of one in 800) was significantly higher than the risk of hospitalization for COVID-19 in randomized controlled trials.17
What VAERS and other reporting systems (including the yet-to-be-referenced and independently evaluated raw data from randomized controlled trials) will miss are potential medium- to long-term harms that neither patients nor physicians will automatically attribute to the drug. For example, if the mRNA vaccine increases the risk of coronary disease within a few months (which was likely a contributing factor to my father's sudden cardiac death), then this would increase the rate of disease well beyond the first few weeks of the jab, but it is very unlikely that this will be attributed to the vaccine later and thus reported.
It is instructive to note that according to ambulance service data, in 2021 (the year of the vaccine rollout) there were about 20,000 (-20% increase) additional calls for out-of-hospital cardiac arrest compared to 2019, and about 14,000 more than in 2020. Data obtained under freedom of information legislation from one of the largest ambulance trusts in England suggests that there was no increase from November 2020 to March 2021, and since then the increase has been seen disproportionately in young people.41 This is a huge signal that certainly needs to be investigated with some urgency.42
Similarly, a recent article in Nature showed a 25% increase in both acute coronary syndromes and cardiac arrests in the 16 to 39 age groups that were significantly associated with administration of the first and second doses of the mRNA vaccines, but no association v.1 with COVID-19 infection.43 The authors state that:
The findings raise concerns about vaccine-induced undetected serious cardiovascular side effects and reinforce the already established causal link between vaccines and myocarditis, a frequent cause of unexpected cardiac arrest in young people. (p. 1)
The disturbing findings in this article have led to calls for retraction. In the past, scientists with a different view of how data should be analyzed would have published an article with divergent assumptions and interpretation for discussion. Now they are trying to censor.
Much more concern has been raised about potential harm from the vaccines in the medium to long term. While some of these concerns remain hypothetical, it may be a serious mistake to focus only on what is measurable and not on the broader picture, especially for young people.
What could be the damage mechanism?
In "conventional vaccines", an inert part of the bacteria or virus is used to "educate" the immune system. The immune stimulant is limited, localized and short-lived. For the COVID-19 vaccines, the spike protein has been shown to be produced continuously (and in unpredictable amounts) for at least four months after vaccination44 and is distributed throughout the body after intramuscular injection.45The spike protein was chosen for the vaccines against the coronavirus of severe acute respiratory syndrome 2 (SARS-CoV-2), possibly because it makes cell entry possible. However, this protein is not inert, but rather is the cause of much of the pathology associated with severe COVID-19, including endothelial damage,46 coagulation abnormalities47 and lung damage.
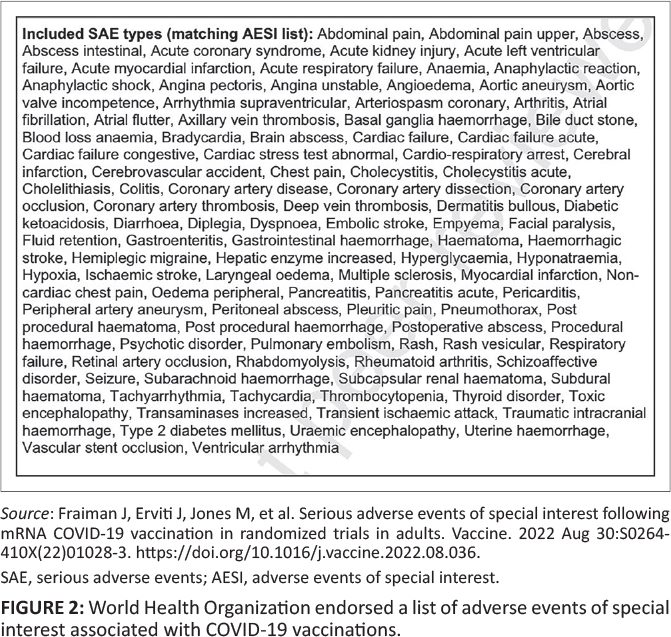
It is instructive to note that before the introduction of the mRNA products, the WHO approved a priority list of potential serious adverse events of particular importance that may occur as a direct result of COVID-19 vaccines.
The list was based on the specific vaccine platform, adverse reactions from previous vaccines in general, theoretical associations based on animal models, and COVID-19-specific immunopathogenesis40 (see figure 2).
Does the vaccine do more harm than good?
The most objective way to determine whether the benefits of the vaccines outweigh the harms is to analyze the effects on "all-cause mortality." This sidesteps the thorny issue of what should be classified as a COVID-19 death, and also fully takes into account any negative effects of the vaccine. It would be surprising to say the least if, during a seemingly deadly pandemic, it could not be clearly and unequivocally demonstrated that an effective vaccine reduces all-cause mortality.
Pfizer's pivotal mRNA trial in adults showed no statistically significant reduction in all-cause mortality, and in absolute numbers, there were even slightly more deaths in the treatment arm than in the placebo group.
Work by Fenton et al. showed an unusual spike in mortality in each age group of the unvaccinated population, coinciding with the vaccine rollout for each age group.48 The rapid decline in the size of this population means that a small time difference could theoretically artificially cause this effect. An alternative explanation is the (more likely) possibility that a rise in post-vaccination mortality was mistakenly attributed to the unvaccinated population: in other words, those who were counted as "unvaccinated deaths" would in fact be those who had died within 14 days of vaccination (a freedom of information [FOI] request has now confirmed that authorities in Sweden recorded deaths within 14 days of vaccination as unvaccinated, creating a misleading picture of efficacy versus mortality).
It is possible that the excessive cardiac arrest and the continued pressure on hospitals in 2021/2022 from non-COVID-19 admissions all point to a non-COVID-19 health crisis that is exacerbated by interventions, which of course also include lockdowns and/or vaccines.
Given these observations and the reassessment of the data from randomized controlled trials of mRNA products, it seems difficult to argue that vaccine adoption has been net beneficial across all age groups. While it can be argued that the vaccines have saved some lives in the elderly or otherwise vulnerable groups, this seems questionable at best for other sections of the population, and when the potential short-, medium- and unknown longer-term harms are taken into account (particularly for multiple injections, for which there is simply no solid safety data), the introduction to the entire population seems at best a reckless gamble. It is important to recognize that the risk of adverse reactions to the vaccine remains constant, while the benefits diminish over time, as new variants are (1) less virulent and (2) do not target an outdated product. After reviewing the data, it remains a real possibility that my father's sudden cardiac death was related to the vaccine. A pause and reconsideration of the vaccination policy for COVID-19 is long overdue.
Again the link to the original english article.
For Part 2 of the paper, click here
https://www.theatlantic.com/science/archive/2022/09/mrna-covid-vaccine-booster-lymphoma-cancer/671308/
There are many n=1 stories but no one follows it through. "Extremely rare cases", "Ultra rare" – anything to not dampen the willingness to get vaccinated...
It always starts with N=1. Sometimes it ends in a dead end; Sometimes it is the first sheep.
We'll see. https://link.springer.com/article/10.1007/s00428-022-03400-w
What kind of bullshit is this?
Just take the 2nd sentence: "Scars on my arm (???)… deadliest diseases such as mumps, measles, rubella (???)"
This article is not to be taken seriously at all.
I have those scars too. Is it too personal and therefore unscientific, you mean?
In terms of form, it is more of a substantiated blog than an old school study. This makes it very accessible, which is also a quality.
I don't know why you wouldn't take a good blog article seriously. I could understand that an editorial board of a scientific journal wants to get rid of that personal touch. Before you know it, your magazine is full of whining stories.
I personally think it is valuable because it reflects the bias that you can take into account when interpreting. The analysis holds up well.
What a strange reaction. The article is full of facts and figures. Why such a strange clincher about 1 sentence? Why is it unacceptable for people like Theo that there are others who criticize the dominant narrative? Do you regret that you had it vaccinated with a barely tested vaccine? Please comment on the content of the data. All the figures (not just this article) that I see indicate that the government measures, including vaccinations, have had 0 effect at best.
The essence of the article is m.i. dat people have never been properly informed about the pros and cons of these vaccines. Your response fits exactly into that picture. You like to be vaccinated with a vaccine without knowing the underlying facts? Excellent. But why such a primitive reaction to this article?
@Cees Mul: You draw completely wrong conclusions about my person. I am not vaccinated. Not against Covid19, and I also let the annual flu shots pass me by.
My qualification 'bullshit' against this article stems from the fact that a cardiologist is going to tell you what vaccinations are, a subject he shows to know little more about than the 1st interested citizen with any intelligence. And that is abundantly clear from what he writes under the heading Vaccines save lives. There is very little good of this. And if you don't understand that, then I dare to conclude that you don't know much about vaccinations either.
I would like to tell Anton that a doctor who dares to count mumps, measles and rubella among the deadliest diseases in the world is really not to be taken seriously. I am of an age when you were not vaccinated against these diseases. You got it 'just' as a child and then you were immune to it for the rest of your life. And furthermore what you say, it is mainly an emo story. Whereby the author cannot dispel the impression that if his father had not died so tragically, he would still have been an enthusiastic defender of the vaccines.
He mentions, with the CFR in parentheses according to Wikipedia – sorry I didn't find another source so quickly:
– smallpox (30%, other forms 95%)
– tuberculosis (43%)
– measles (1-3%)
– mumps (1% but meningitis and deafness) and
– rubella (mild but very serious for unborn children).
They are indeed not the deadliest but still very deadly or debilitating diseases and are easily transmissible. That combination may justify the term "deadliest" as in "most deaths".
There are also diseases that are 100% fatal, but if hardly anyone catches them, they are not much in terms of risk.
I don't think that "inaccuracy" is enough to dismiss the story accordingly.
@Theo. Thank you for explaining. I myself am 60+, have never taken a flu shot and certainly not a Covid 'vaccine'. I have been forced to read a few things about virus infections in recent years. I see Malhotra's comments about other vaccinations more as an introduction. Probably to cut the grass from under the feet of critics in advance (otherwise someone will immediately be put in the corner of antivaxxers, and that is not so relevant to this discussion).
The fact that he is a cardiologist does not seem to me to be a reason to doubt his findings. It is mainly about studies that compare the ratio between risk of Covid death and the side effects of the vaccines.
The fact that the death of his father has made him doubt the government's approach is also not very relevant. I myself have not believed the story from the beginning, and have always relied on natural immunity. Others come to an understanding later, for whatever reason. Better late than never, I would say.
I think the essence of his argument is that the risks of Covid-19 (and all its variants) have been systematically exaggerated by governments, while the risks of the vaccines have been systematically reduced. Hugo de Jonge: "these vaccines are 100% safe". Now that's Bullshit. As a result, many people have been persuaded under false pretenses to accept an Mrna vaccine. That is particularly bad.
I am glad that someone like Malhotra is publicly questioning the vaccination drive. It seems to me that anyone with a critical view of mass vaccination (and we seem to agree on this) should be happy with a publicly known figure who denounces this.
I think he wants to indicate with the scars the number of vaccines he has been administered to indicate how he stands in the whole vaccine discussion. As far as that is not already apparent from the text. After all, reading comprehension is also quite an art.
Article is intriguing to say the least and many studies like this will follow. The "new world Order" should ring a bell, as it did in 2009 with the vaccine against the swine flu.
If you think it's bullshit, you should take the next shot as well. Nothing happens to you, does it?
I assume that "Theo" is a troll.
I don't take that for granted. In my own circle of friends and acquaintances, I know doctors of integrity who react exactly the same way.
I think the link at part 2 (halfway through this page) should be this: https://insulinresistance.org/index.php/jir/article/view/72/228
That was the link to Part 1, that was indeed not logical so I understand the confusion. I have adjusted it. Thank you!
Oh dear. After Robert Malloot, we now have Aseem Malle Hoaxer. Respected cardiologist...
https://snowdon.substack.com/p/the-downward-spiral-of-aseem-malhotra?utm_medium=web
That with that award is indeed a strange stunt. Very stupid... You would almost think of a failed joke.
In terms of content, I think what he says makes sense (also when it comes to fat and sugar, he is not the only one who thinks so). By the way, that substack criticizes him also contains things that are not right, as soon as it becomes substantive.
I still think he knows how to create a strong, coherent and substantiated story.
The bottom line: as long as there is no openness of data, we cannot rule out that the vaccines contribute to excess mortality. The fact that these data are constantly kept secret suggests the worst. He nicely reinforces the call for transparency and independent evaluation.
But indeed, 'respected' is not good. I made it 'controversial'.