
This part 2 of the paper by Aseem Malhotra, I added afterwards to the post of Part 1, of September 26. That post became very long and early readers may have missed it. That's why I decided to write a separate article, also because there seems to be quite a bit of dust on it. In this part, the focus is on the failing system.
Below is the translation of Part 2
Part 2: A pandemic of misinformation
What has become clear with regard to the coronavirus 2019 (COVID-19) vaccines is that we are dealing with a pandemic of misinformed doctors and a misinformed and unintentionally harmed public. The coercive imposition of these COVID-19 vaccinations (certainly not evidence-based policies) was a particularly egregious misstep, especially in light of clear indicators suggesting that the use of these pharmaceutical interventions – especially in younger age groups – should have been suspended. Such policies continue to undermine the principles of ethical evidence-based medical practice and informed consent, at the expense of optimizing patient outcomes.
In his 2017 paper, 'How to survive the medical misinformation mess', Professor John Ioannidis and colleagues emphasise that:
Most clinical trial results are misleading or not helpful to patients. Most guidelines (on which many doctors rely to make treatment decisions) do not fully acknowledge the poor quality of the data on which they are based. Most medical stories in the mass media do not meet criteria for accuracy, and in many stories, the benefits are exaggerated and the disadvantages are minimized.1 (p. 1).
A senior physician who is in regular contact with the Chief Medical Officer of the United Kingdom (UK), Professor Chris Whitty, recently expressed to me his concern that he believes that most of his colleagues in leadership positions influencing health policy do not critically assess the evidence and instead rely on media narratives about COVID-19 and the vaccine. This is consistent with the admission of Rochelle Walensky, the former president of the Centers of Disease Control (CDC), whose optimism about the efficacy of Pfizer's COVID-19 vaccine stemmed from reading a CNN news report, which was an almost verbatim reproduction of Pfizer's own press release.2
Has the British Chief Medical Officer Professor Chris Whitty critically assessed the evidence? Recently, he publicly shared a letter3 in which he indicated the importance of healthcare workers getting vaccinated against COVID-19. This letter was not complete and did not match the overall evidence: "The COVID-19 vaccines are safe and effective". It would have been more accurate to state that "the vaccine is not completely safe and not nearly as effective as we had hoped. Not even in the same neighborhood as the effectiveness and safety of traditional vaccines".
Professor Chirs Witty stated:
Our professional responsibility is to get the covaccines as recommended to protect our patients".3
He should have said that as far as omicron is concerned, "the vaccine offers little to no protection against infection". Data on the delta variant also shows that, once infected, there is no significant difference in transmission rates between the vaccinated and the unvaccinated.
Professor Whitty's statements are especially surprising because the CEO of Pfizer has stated that in relation to omicron "we know that the two doses of a vaccine provide very limited protection, if there is protection at all".5
Could it be that Professor Whitty is also a victim of medical misinformation?
There are four main motivations and seven sins that underlie the medical misinformation:
Motives:
- Much published medical research is not reliable or is uncertain, does not benefit patients or is not useful to decision-makers;
- Most health professionals are unaware of this problem;
- Even if they are aware of this problem, most health professionals lack the skills necessary to assess the reliability and usefulness of medical evidence; and
- Patients and families often lack relevant, accurate medical evidence and expert guidance at the time of medical decision-making.1
Sins:
- Bidental research funding (that is, research funded because it is likely to be profitable and not beneficial to patients).
- tendentious reporting in medical journals
- tendentious media coverage
- Biased patient leaflets
- Commercial conflicts of interest
- Defensive medicine
- The inability of doctors to understand and communicate health statistics.6
Ioannidis and colleagues emphasize that:
"The ignorance of this problem, even at the highest levels of academic and clinical leadership, is profound"1.
Combined over several decades, these upstream and downstream risk factors for misinformation have had a devastating effect on the healthcare system in which we now find ourselves. Over-prescribing drugs is considered such a public health threat that in the past 10 years, two leading medical journals (the BMJ and JAMA Internal Medicine) have launched campaigns to limit the harms of too much medical intervention.
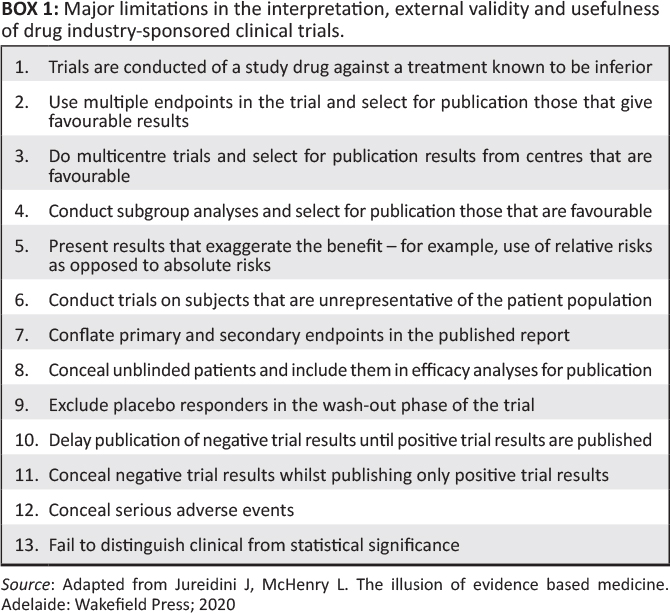
According to the co-founder of the Cochrane Collaboration, Peter Gøtzsche, prescription drugs are the third leading cause of death worldwide, after heart disease and cancer.7 This is not surprising when one realizes that most of the published research is misleading, especially when the benefits of drug research are exaggerated and the adverse effects of too many drugs are underestimated. (Box 18).
If a doctor makes clinical decisions based on biased information, it leads (at best) to suboptimal outcomes and (more worryingly) to harm to the patient.
Shortcomings of the medical profession
According to Professor Carl Heneghan, an emergency medicine physician and director of the Centre of Evidence-Based Medicine at the University of Oxford, "with every procedure you do as a doctor, you have to ask yourself two questions: how much difference does it make? How do I know?" 9
Building on the Academy of Medical Royal Colleges' Choosing Wisely campaign,10 it is instructive to note that in 2020 the General Medical Council issued guidelines on the duty of physicians to engage in shared decision-making with patients, underpinned by informed consent.11
There are six essential components of informed decision-making: (1) description of the nature of the decision; (2) discussion of alternatives; (3) discussion of risks and benefits (in absolute terms); (4) discussion of related uncertainties; (5) assessment of patient understanding; and (6) eliciting patient preference.
If the vaccine has not been administered in accordance with these principles (which is likely to be done on a large scale, in accordance with historical data)12)), then this is also a significant breach of the duties of a doctor of the General Medical Council to 'give patients the information they want or need in a way that they can understand'.13
It is instructive to note that the greater the financial interests in a particular field, the less likely it is that the research results will be true.14 As already demonstrated in Part 115 of this article, mandating a new emergency use vaccine for non-vulnerable people has little to no effect on preventing infection and severe disease, therefore has no scientific validity and therefore violates the principles of informed consent. However, it greatly increases the manufacturer's profits. By expanding the use of the mRNA vaccine to the majority of the population who are at very low risk for serious complications from COVID-19 but are more likely to experience serious and/or life-threatening side effects such as myocarditis or sudden cardiac death, Pfizer has generated tens of billions of dollars in revenue to date, making it one of the most lucrative products in history. If policymakers had focused more on protecting the vulnerable – and doctors had been given the opportunity to make decisions together with patients based on transparent communication about risks and benefits – patient outcomes would likely have improved significantly,16 But the profits of the pharmaceutical companies would probably have been a fraction of what they actually yielded. As former editor of the New England Journal of Medicine Dr. Marcia Angell previously noted, "the real battle in health care is one of truth versus money."17
Institutional corruption and erosion of public trust
Institutional corruption is defined as the deviation of an institution from a baseline of integrity.18 There is a long documented history (both through studies and lawsuits) of the strategies by which drug companies hide, ignore, or misrepresent evidence about new drugs. Distortion of the medical literature and misrepresentation of data by companies looking to expand the market for their product can lead to over-prescribing, with the predictable result that millions of patients suffer from preventable side effects.
Before 2020, there were already gross shortcomings in the medical-industrial complex – there was too much influence from the pharmaceutical industry on clinical decision-making. This has not gone unnoticed, resulting in a growing crisis of confidence in medical research: a report by the Academy of Medical Sciences in 2017 found that 82% of GPs and 63% of the public did not believe that the results of pharmaceutical industry-sponsored research were unbiased.19Also, only 37% of the public trust medical research, compared to 65% who trust the experience of their friends and family.20
This growing lack of trust – recently exacerbated by coercion, vaccine passports and little mainstream media coverage of an unprecedented scale of reported vaccine harms among the population – was recently exemplified by the refusal of 8 million people in the UK to take the COVID-19 booster vaccination. Moreover, all the focus on COVID-19 (which poses virtually no risk to children in its current omicron form) diverts attention from, and even worse, raises suspicions of more effective and safe interventions such as the measles, mumps and rubella (MMR) vaccines. In the United Kingdom, MMR vaccination coverage has reached its lowest level in ten years.
Regulatory failures and investigative misconduct
The authorities want the public to "trust the science," but vaccine manufacturers have successfully made agreements with several major governments around the world that shield them from financial liability in the event of vaccine-related damage. Interestingly, India, the largest democracy in the world, denied Pfizer harmless relief for its vaccine. An Indian government source told Reuters that:
The whole problem with Pfizer is the indemnification. Why should we sign it? If something happens, a patient dies, we can't question them [Pfizer]. If someone files a lawsuit, the central government is responsible for everything, not the company.21(p. 1)
Pfizer preferred to leave the Indian market rather than conduct a local safety and immunity study.22
It's important to first understand that drug companies have a fiduciary duty to make a profit for their shareholders, not a legal responsibility to give you the best treatment. During a lecture at the Centre of Evidence-Based Medicine in Oxford in 2014, Peter Wilmshurst said that the real scandal is that many of those with a responsibility for patients and scientific integrity (doctors, academic institutions and medical journals) often collude with the industry for financial gain.23 It is precisely this industry that has been found guilty of the most egregious corporate crimes: between 2003 and 2016, the 11 largest pharmaceutical companies paid $28.8 billion in fines in the United States (US) alone,24 many of them for criminal activities such as illegally marketing medicines, manipulating results and hiding data on harm. As noted in the BMJ, no systematic changes have been made since then to mitigate this damage.9
In an international survey of respondents from higher education institutions, 14% admitted to knowing a colleague who fabricated, falsified, and altered data, and 34% of scientists reported questionable research practices, including selective reporting of clinical outcomes in published research and the concealment of conflicts of interest.25 One blatantly documented case of research misconduct involved a prominent Dutch physician whose work influenced the European Society of Cardiology's guidelines on the use of beta-blockers in non-cardiac surgery. He was fired from Erasmus University for "violations of academic integrity", including the use of "fictitious data" in the investigation. It is estimated that these guidelines increased the mortality rate of patients by 27%, resulting in 800 000 excess deaths in Europe over an 8-year period.26
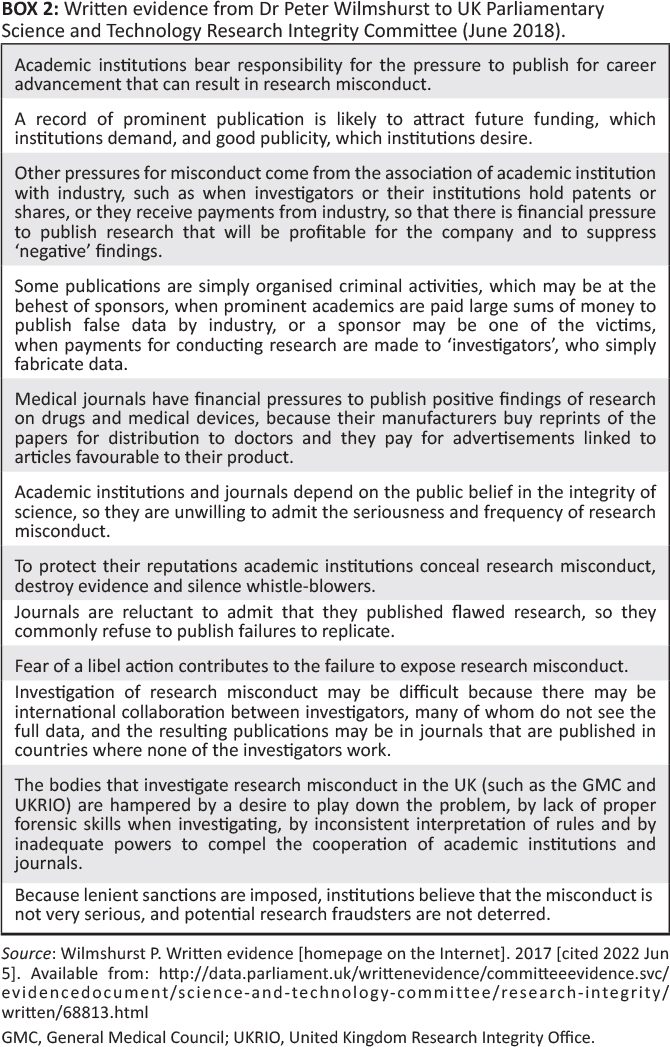
In evidence submitted in 2017 to the UK Parliamentary Committee for the Evaluation of Science and Technology on Research Integrity (chaired by Sir Norman Lamb), Dr Peter Wilmshurst lists a number of risk factors that encourage misconduct in research in UK institutions (see Box 2 27). His solution, which I agree with, would be to ensure that serious forms of investigative abuse are criminalized with meaningful sanctions and that allegations of such activities are investigated by an independent body with legal powers.27
A researcher from a prestigious British institution contacted me to inform me that in his cardiology department, a group of academics deliberately suppressed research showing that the mRNA vaccine significantly increased coronary risk, as determined by cardiac imaging, compared to the unvaccinated. The chairman of the group expressed concern that publication of the data could lead to a loss of funding by the pharmaceutical industry.28 After alluding to this in GB News, the whistleblower informed me that letters of non-disclosure had been sent to all members of the team involved in this particular area of investigation.
Evidence-based medicine and the rollout of the COVID-19 vaccine
Neither the drug authorities nor the vaccine manufacturers have yet shared all the raw data from the pivotal trials for the COVID-19 vaccines.29The raw data from the clinical trials comprise thousands of pages that have yet to be released for independent research. This is important because in the past, independent researchers who were sometimes given access to this data could completely overturn the conclusions of the published trials: An example of this is Tamiflu.30Gaining access to clinical case reports for Tamiflu eventually revealed that the drug was no more effective than acetaminophen for flu and that it also had minor but significant drawbacks. The British government had stockpiled half a billion dollars for a drug that turned out to be useless, despite claims by the manufacturers (Roche, Basil, Switzerland) that it shortened the duration and severity of the disease. The independent researchers who were able to analyze the data concluded that all industry-sponsored research should be considered marketing until proven otherwise.
It is against this backdrop that transparency advocates have sued the Food and Drug Administration (FDA) to access the data on the basis of which Pfizer's vaccine (BNT162b2) was granted emergency use authorization.31 The FDA wanted a U.S. federal judge to give the agency 55 years to release this data.32 Why should the FDA – "responsible for overseeing more than $2.7 trillion in the consumption of food, medical products and tobacco"33 – do this? Secrecy should never shield a public health intervention. The attorney acting on behalf of the plaintiff Aaron Siri reported that:
The government also tried to delay the full release of the data it relied on to authorize this product until nearly every American alive today is dead. This form of government is destructive to freedom and is at odds with the openness that is required in a democratic society.31
Instead, the judge ordered the FDA to release the data over an eight-month period after all commercially sensitive information had been redacted.
A major risk factor for failing to protect the public from such harm is the lack of independence of the regulator. The FDA's Center for Drug Evaluation Research (CDER) receives 65% of its funding from the pharmaceutical industry (primarily in the form of user fees).34 For example, as part of the approval process for its COVID-19 vaccine, Pfizer made in May 202135 a transfer to the FDA of $2,875,842 under the Prescription Drug User Fee Act of 1992.36Full FDA approval for Pfizer's COVID-19 injection followed in August 2021.37, despite recent evidence that the original RCT data indicated a greater risk of serious adverse reactions to the vaccine than to hospitalisation due to COVID-19.
Separate analyses have shown that the vast majority of new drugs approved by the FDA in recent decades were later found to be just copies of old drugs, which is not surprising when one realizes that drug companies spend 19 times more on marketing than on research on new molecular entities, all of which contribute to significant waste. Between 2000 and 2008, only 11% of the 667 FDA-approved drugs were found to be truly innovative. In the US, it is estimated that 30% to 50% of healthcare activities do not provide any benefit to patients. A survey of FDA scientists found that 70% of them felt the FDA lacked the resources to fulfill its mission of "protecting public health... and help the public get accurate, science-based information to use medicines and foods to improve their health" effectively.38
An analysis of every new drug approved in France between 2002 and 2011 showed that only 8% offered any benefit and that double that – 15.6% – turned out to be more harmful than beneficial, while the majority of other new drugs were essentially copies of old drugs and contributed to a colossal waste of public money.18Similar conclusions have been drawn in Canada and the Netherlands. In my view, the evidence is overwhelming that the overall net effect of the pharmaceutical industry on society and public health over the past few decades has been very negative.
COVID-19 vaccination in persons at lower risk
Regardless of the benefits of inoculating higher-risk groups, where a small but significant benefit may exist against the original Wuhan strain, inoculating lower-risk children in the name of preventing asymptomatic transmission does not have strong scientific validity and therefore exposes them to potential harm.
In the United Kingdom, the Office for National Statistics has disclosed an as yet unexplained significant increase in deaths among 15- to 19-year-old children since May 2021 compared to the five-year average. Has the COVID-19 vaccine been ruled out as a possible cause, given what we now know about potential harm, especially with regard to myocarditis, myocardial infarction, and sudden cardiac death (even in 16- to 39-year-olds)?39
In September 2021, the Joint Committee on Vaccination and Immunisation (JCVI) issued a controversial recommendation that the Pfizer/BioNTech vaccine is marginally beneficial for 12- to 15-year-old children.40The Medicines and Healthcare products Regulatory Agency (MHRA, the UK equivalent of the FDA) had previously stated that:
They carefully reviewed the clinical trial data of the Pfizer/BioNtech vaccine in more than 2,000 children aged 12-15 years and concluded that the benefits of this vaccine outweigh the risks and that it is effective and acceptably safe in this age group [...] No new adverse reactions were identified and the safety data in children were similar to those of young adults. As in the young adult age group, most adverse reactions were mild to moderate and related to reactogenicity (e.g. sore arm and fatigue).41(p. 1)
Is this in line with the overall evidence?
Award-winning investigative journalist Maryanne Demasi published the harrowing story of one of the trial participants, 12-year-old Maddie De Garay. After severe abdominal pain followed by seizures, she was admitted to the hospital and now she is permanently disabled, wheelchair-bound and fed via a nasogastric tube. In Pfizer's study, they reported her side effect as mild: stomach upset.42
It is important to emphasize that the risk of death from COVID-19 in a 12- to 15-year-old is close to zero, at 1 in 76,000. In accordance with the principles of ethical, evidence-based medical practice through shared decision-making, parents should be told that there is no high-quality data showing that the vaccine in children prevents infection, transmission, serious illness or death, but that it can have serious side effects such as myocarditis – especially in young men, where it occurs in 1 in 270043 – and severe disability.
Can financial interests influence the recommendations?
On its website, the MHRA states that the majority of its funding comes from the pharmaceutical industry and 3 million pounds (British pounds) from the Bill and Melinda Gates Foundation (BMGF). Are policymakers and the public aware that the foundation's share capital is heavily invested in food products (including McDonald's and Coca-Cola) and pharmaceutical companies, directly and indirectly? As a 2009 Lancet paper notes, funders' priorities are often determined by personal interests rather than the recipient country's priority health interests.44 "The BMGF's portfolio of pharmaceutical companies deserves attention given Mr. Gates' personal belief in the role of patents as a driver of innovation in the field of pharmaceuticals and medical technology."45
Obesity researcher Dr Zoe Harcombe has also examined the financial ties that may influence the position of the Joint Committee on Vaccines and Immunisation and found that the members of the subcommittee work for organisations that receive a total of $1 billion from the BMGF.46 It is also worth noting that Professor Wei Shen Lim, Chair of the JCVI Subcommittee on Vaccines, is directly responsible for the material funding his department receives from Pfizer.47 This in no way suggests that the JCVI has acted incorrectly, but when trust in an organisation such as the JCVI is necessary, it is essential that there is no perception of conflicts of interest. The systems for selecting panelists, examining evidence, and the methodology and openness of their recommendations must be impeccable.
The most direct cause of harmful health outcomes: Corporate power and the commercial determinants of health
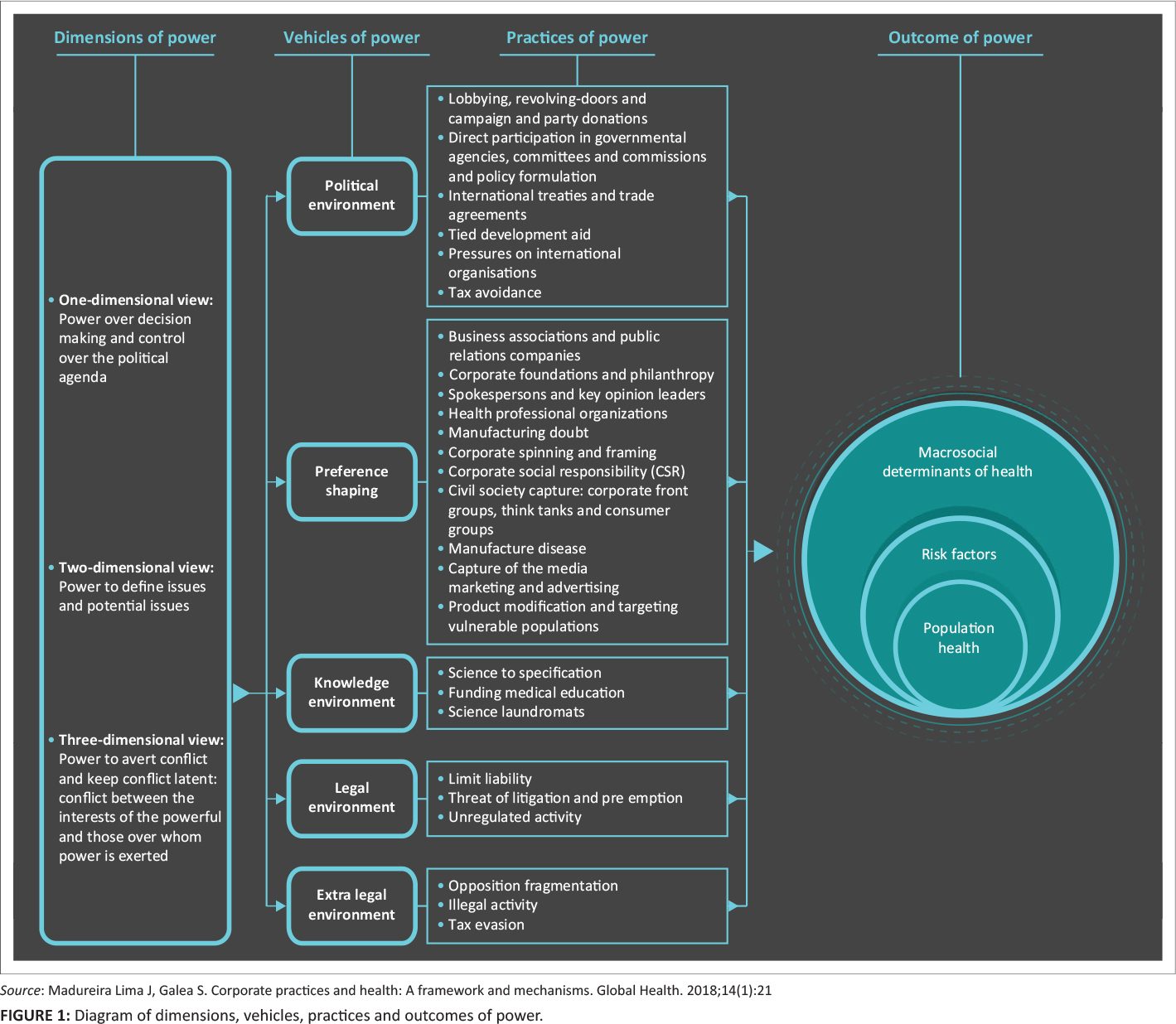
The commercial determinants of health are best defined as "private sector strategies and approaches to promote products and choices that are harmful to health".48Corporations exercise their power through a combination of factors, including intellectual exploitation. This includes the ability to determine the dominant narrative, establish the rules and procedures by which society is governed, determine the rights, living and working conditions of ordinary people, and appropriate knowledge and ideas49 (see figure 145).
In the case of the mRNA vaccine, Pfizer seems to have benefited at least to some extent from this corporate framework strategy by shaping the knowledge environment (Pfizer was responsible for the design and conduct of the trial, the data collection, the data analysis, the data interpretation and the writing of the manuscript), the political environment (lobbying), the formation of preferences (corporate foundations and philanthropy, spokespersons and key opinion leaders, influencing the media), the legal environment (limitation of liability) and the extra-legal environment (fragmentation of the opposition by removing critics of the current dominant narrative that the vaccine is safe and effective).45
As a result, it has earned tens of billions of dollars from a product that is extremely ineffective compared to proven traditional vaccines and most other drugs and contains unprecedented reports of serious harm.
Distorted media coverage and censorship of legitimate scientific debate
Companies are able to form preferences and shape the dominant narratives about the determinants of health, through unchecked invisible power. One way is to own mass media. The global media market is dominated by seven companies and chains that own 80% of the newspapers in the US.50 The BMGF's grants to global media companies are notable – for example, The Guardian Media Group has received more than $12 million in grants from the BMGF over the past 12 years. The control of advertising in the print and broadcast media also influences editorial decisions. Most health journalists (including a few I have spoken to) are generally unaware that the information they obtain for their stories has been deliberately shaped by the private interests of manufacturers and "research" universities.
The BBC, while seemingly not directly influenced by industrial interests, has traditionally been seen by some as the most reliable media source in the UK. Her coverage of issues surrounding COVID-19 has been extremely poor in my view (possibly due to additional pressure from the government) and – specifically on issues surrounding the vaccine – grossly careless. During a recent report on tennis player Novak Djokovic explaining his decision not to take the vaccine until he has more information about its benefits and harms, a reporter asked the question "how much more information does he need?". The reporter failed to mention that Djokovic has had COVID-19 and that there is evidence that natural immunity provides significant protection against reinfection and severe disease, and that systemic side effects are nearly three times as likely in people with natural immunity who are subsequently vaccinated.
Further, the BBC has falsely portrayed a guest of popular podcast host Joe Rogan, Dr. Robert Malone, as a "known anti-vaxxer, who opposes vaccinating children," without mentioning that Dr. Malone is a co-inventor of the technology that led to the vaccine, has worked in vaccine development for 20 years at the U.S. government level, and was one of the first to actually offer two shots of the vaccine. Moderna jab. The BBC also curiously failed to publish one of the most important stories about the pandemic in one of the most respected and influential medical journals in the world: An investigation by the BMJ uncovered evidence of bad practices at a contract research company involved in Pfizer's pivotal COVID-19 vaccine research. A regional director at one of the trial sites in Texas, USA, documented evidence that Pfizer falsified data, failed to blind patients, employed inadequately controlled vaccinators, and was slow to follow up on adverse events. The same day she emailed her complaint to the FDA, she was fired.51 She then filed a fraud lawsuit against Pfizer on behalf of the U.S. government (and the people of the U.S.) under whistleblower law. Pfizer's motion to dismiss the case (which apparently failed to convince the judge) was based on the fact that the FDA had not responded to its (or other) complaints, so the allegations were of no concern to the government.
In the US, Senator Ron Johnson, who held hearings with health professionals who presented data on clear, substantial, and very common side effects of the mRNA jabs that deserved widespread public attention, said that "the mainstream media are co-conspirators in this political dirty trick. Will they be held accountable for their role in this deception?"52
Social media platforms remain guilty of spreading disinformation. Due to their business model, which is aimed at increasing engagement at all costs, society is increasingly losing access to the truth and deteriorating our capacity for empathy as individuals, creating even more division and hostility. The so-called "fact checkers" have censored everything that questions the prevailing mainstream narrative (the establishment is reliable and the vaccines are completely safe). They even labeled the BMJ's investigation into possible fraud in Pfizer's pivotal trial as disinformation and stopped users from sharing the story on their platform. A letter from the magazine's current and former editor-in-chief to Mark Zuckerberg questions the integrity of Facebook's fact-checkers:
Rather than investing a proportion of Meta's substantial profits to help ensure the accuracy of medical information shared through social media, you apparently delegated responsibility to people incompetent in carrying out this crucial task.53(p. 1)
It has also come to light that Facebook has partnered with drug company Merck to decide what content to censor on its platform in relation to COVID-19 and the vaccine.54 Is Facebook aware that Merck has paid one of the largest fines in U.S. history for being found guilty of fraud related to their painkiller Vioxx?55 Not only did one study find that the drug did not reduce stomach bleeding (their original main selling point) compared to ibuprofen, but it also significantly increased the risk of heart attacks and strokes, causing an estimated 40,000 to 60,000 additional deaths over a five-year period.56
Improving metabolic health
The lack of public health messaging and policies to help people improve their lifestyles during the pandemic is a missed opportunity to mitigate the harms of respiratory diseases like COVID-19. After age, obesity and conditions related to excess body fat are the biggest risk factor for worse COVID-19 outcomes. More than 90% of deaths from COVID-19 occurred in countries where more than 50% of the population is overweight or obese. The United Kingdom's biobank data during the first wave showed a more than four times higher risk of hospitalization due to COVID-19, depending on lifestyle factors. For example, a non-smoking adult in their mid-50s with a normal body mass index (BMI) and adequate exercise had a 1 in 1,521 chance of being hospitalized after contracting COVID-19, while an obese, smoking, sedentary person's risk was 1 in 327.57
The hypothesized pathophysiological mechanisms of the risk and complications of an infection include a series of markers that cause insulin resistance and chronic inflammation.
Even a single high blood glucose reading in non-diabetics (a marker of insulin resistance) who are hospitalized has been found to be associated with worse outcomes.58
Recently, it has also been found that in the UK, of the 175,256 deaths associated with COVID-19 (2020-2021), less than 10% (17,371) had COVID-19 as the sole cause on the death certificate, suggesting that the risk of COVID-19 for individuals with optimal metabolic health (Figure 259) was significantly smaller, according to the results of the above-mentioned UK biobank study.60
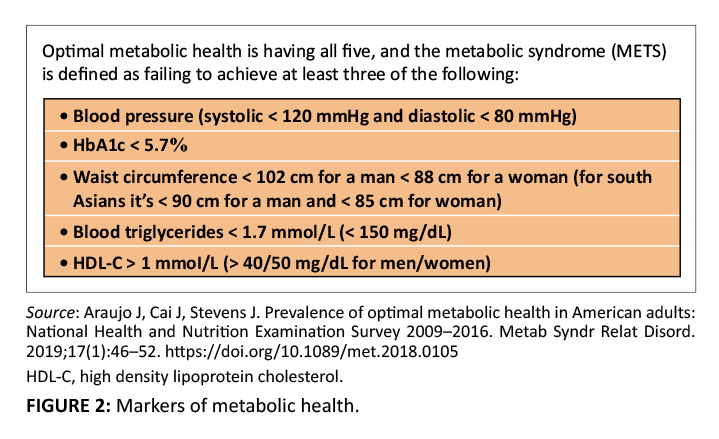
The government and medical authorities should have prioritized emphasizing the importance of eliminating ultra-processed foods and low-quality carbohydrates to reduce the risk. They could have pointed out to the audience that it has been shown that the reversal of metabolic syndrome can occur in up to 50% of patients – independent of weight loss – within four weeks just by changing the diet.61
The coronavirus disease 2019 was a short-lived crisis that took advantage of a slow pandemic of poor metabolic health (see Figure 259), which is also the main cause of the major chronic diseases that have been putting increasing pressure on healthcare systems around the world for decades. It is estimated that a healthier lifestyle (in absolute terms) could eliminate 40% of cancer cases and 75% of cases of cardiovascular disease and type 2 diabetes.63
Optimal metabolic health would not only improve the immune system's resistance, but also reduce the burden of heart disease, type 2 diabetes, cancer, and dementia.
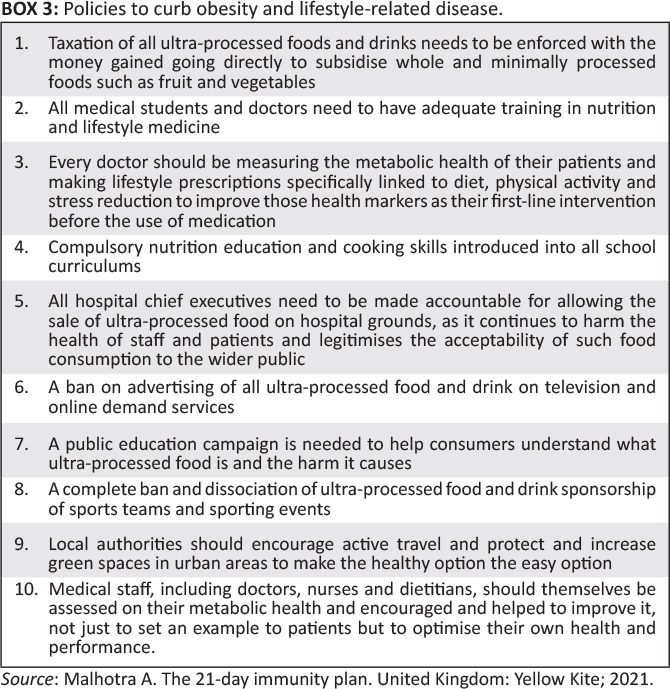
Learning lessons from tobacco control: policy changes addressing the availability, acceptability and affordability of highly processed foods and beverages and low-quality carbohydrates would significantly reduce the burden of obesity and related metabolic diseases and are likely to optimise the population's immune resistance within a few years (see Box 362).
The solutions
There was never any evidence that COVID-19 justified vaccination mandates, passports, or any of the other coercive measures taken by various governments worldwide. Every patient who was offered a COVID-19 vaccine should have known what their risk of COVID-19 is, depending on age and risk factors. In accordance with ethical medical practice, doctors should have informed patients that their absolute risk reduction for infection with the previous, deadlier variant is about 0.84% or 1 in 119 (based on non-transparent data) and that this level of protection lasts only a few months. They should also have provided more accurate and robust data on what is the actual absolute individual risk reduction of COVID-19 death from the vaccine, what the actual rates of serious adverse events (such as permanent disability, hospitalization or death) are. Only when doctors and patients have all this information can they be able to have frank conversations about whether a treatment – including this vaccine – is the right one for them.
The profession should explain that optimizing metabolic health gives patients the best chance to ensure that they are not only resistant to infection, but also reduce their risk of chronic diseases such as heart disease, cancer and dementia.
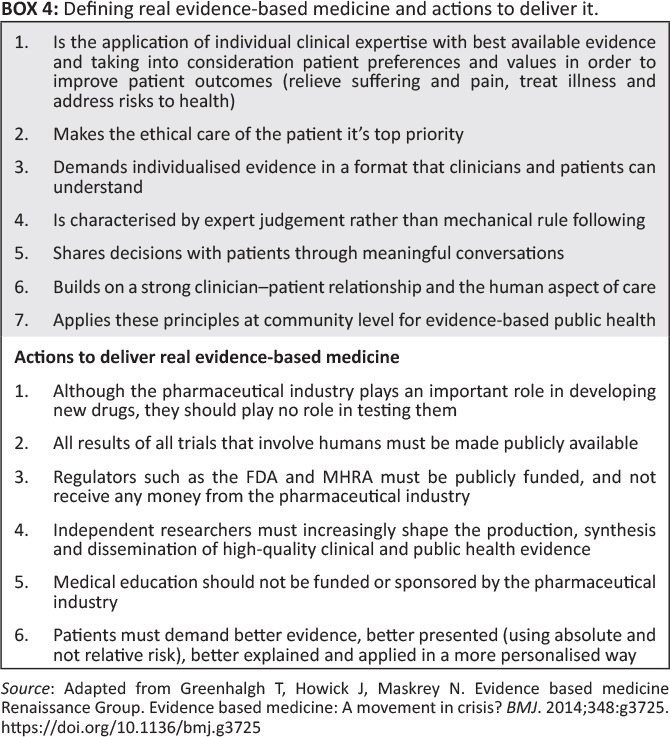
The time has come to prevent misleading evidence from entering the media and clinical decision-making and resulting in unethical and unscientific policy decisions. It is time for real evidence-based medicine (Box 464).
There are also strong scientific, ethical, and moral arguments for halting the current administration of the mRNA vaccine until Pfizer releases all raw data for independent research.30This will provide a more accurate picture of the groups that are more likely to benefit from the vaccine than the groups that are more likely to be harmed.
Given all the recent well-documented above-mentioned shortcomings in the integrity of medical research (including that possibly half of the published medical literature "may simply be untrue"), Lancet editor Richard Horton wrote in 2015 that science has taken a turn into darkness and asked who was going to take the first step in cleaning up the system.65 The unprecedented rollout of an emergency use vaccine without access to the raw data, with mounting evidence of significant harms, exacerbated by mandates that seem to serve no purpose other than to support drug industry profits, have exposed the worst failings of modern medicine on an epic scale, with additional catastrophic damage to public health confidence.
We should use this as an opportunity to transform the system into better doctors, better decision-making, healthier patients and restoring confidence in medicine and public health. Until all raw data on the mRNA COVID-19 vaccines have been independently analyzed, claims that they provide a net benefit to humanity cannot be considered evidence-based.
Credits
I thank Dr. Clare Craig for edits and data analysis, and Alex Starling for comments and suggestions. The author is also grateful for the help of a scientist who wishes to remain anonymous due to career pressure.
Competing interests
The authors state that they have no financial or personal relationships that could have inappropriately influenced them in the writing of this article.
Author's contribution
A.M. is the sole author of this article.
Ethical considerations
This article followed all ethical standards for research without direct contact with human or animal subjects.
Financing information
This study did not receive a specific grant from a funding agency in the public, commercial or non-profit sector.
Data availability
Data sharing does not apply to this article, as no new data was created or analyzed in this study.
Disclaimer
The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of any body affiliated with the author.
Again the link to Part 2
What a TOP article, the crowning glory of your work Anton! It will have taken you many hours and days to produce this, thank you very much for all your efforts!
I only translated it. That was a bit of work, but not days! We owe the real work to Dr. Aseem Malhotra.
Off topic, but perhaps interesting for visitors of this site: a lecture by a British professor of statistics for whom I already had strong admiration before Covid and who has remained just as rational as Anton.
https://media.ed.ac.uk/media/1_k4ksrgbr
Fantastic!!! The ease with which that man talks you through those formulas... And then the discussion at the end, great. The statistics are way over my head. But jazz sometimes does that too and yet you can hear whether it is right or not. Enjoy!