
Excess mortality should be considered normal. It's now about whether you have the greatest excess mortality or -nice puh- less excess mortality than another country. At least that's how it seems, after a statement by someone in Bar laat, who apparently had slipped through the editorial screening. He claimed that the Netherlands had the most excess mortality in all of Europe. Of course that is not possible.
The Netherlands is not at the top, that is simply not right. In the program itself, all the 'journalists' are of course looking like rabbits in the headlights - no one has a clue. But: in fact, something like that should not be said in the media at all. That screening error at Bar Laat must of course be corrected immediately! Imagine, you miss a grant or you get penalty points from the medical-military complex or Ab Osterhaus gets angry! Who do you call as a fact checker? CBS!
CBS spokesperson Prof. Dr. I.A. (Ruben) van Gaalen spoke about the position of the Netherlands in the European excess mortality competition, on Radio 1 during 'Fact or Fiction':
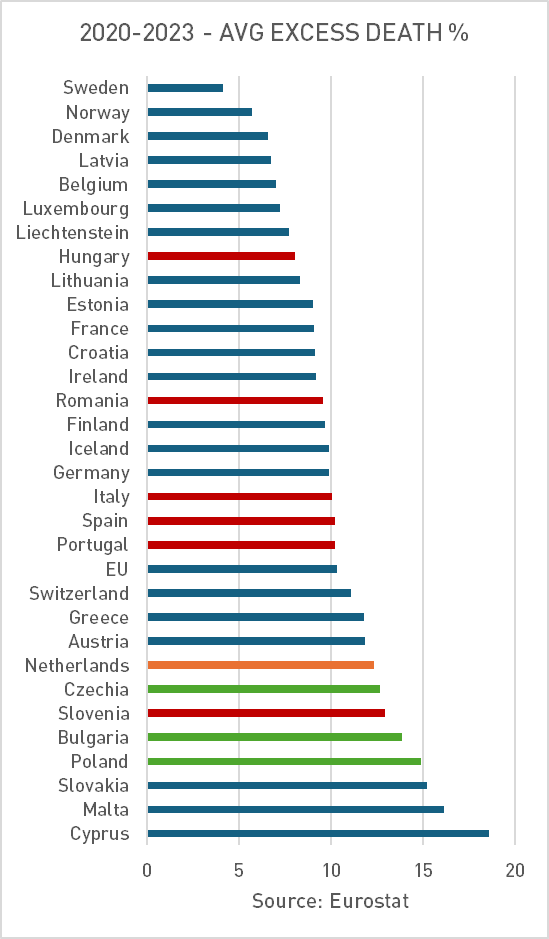
"Als je op uniforme wijze berekent hoe hoog de oversterfte was in die periode (2020-2023), dan zie je dat Nederland een middenmoter is. Het is zeker dat er veel extra sterfte was, dus de oversterfte was er inderdaad maar het is niet zo dat Nederland helemaal bovenaan staat."
"Er zijn legio landen zoals Portugal, Spanje, Engeland, Tsjechië, Polen, Italië, Hongarije, Roemenië en vooral Bulgarije die een veel hogere oversterfte hadden in die periode.
Een lagere oversterfte hadden België, Duitsland, Slovenië, Ierland, Frankrijk, Zweden, Noorwegen, Denemarken dus: Nederland zit daar gewoon tussenin."
So much for Ruben van Gaalen's fact check. Let's take a look at the official figures on Eurostat. From the European Commission, of course, so completely unsuspected. 😉
Fact or fiction?
If we look at Eurostat, Ruben guessed right three times (the green bars) and 6 times wrong. He did not mention the blue bars.
Hij gaat ook maar tot (en met) 2023. Maar ze hebben het in de radio-uitzending over "de coronaperiode", die was in 2022 al voorbij.
De cijfers t/m november 2024 zijn er ook inmiddels, dus als voorlichter had hij die er zeker bij moeten betrekken. Je wil de bevolking toch op de hoogte houden, nietwaar. Maar in 2024 zie je dat Nederland alleen maar verder wegzakt in de poel des doods. En dat klopt niet met de oversterftemeldingen van onze overheid. Dus dat hou je dan achter. En de PR-ambtenaren op het mediapark slikken het voor zoete koek. Want "het is een instituut, hè."
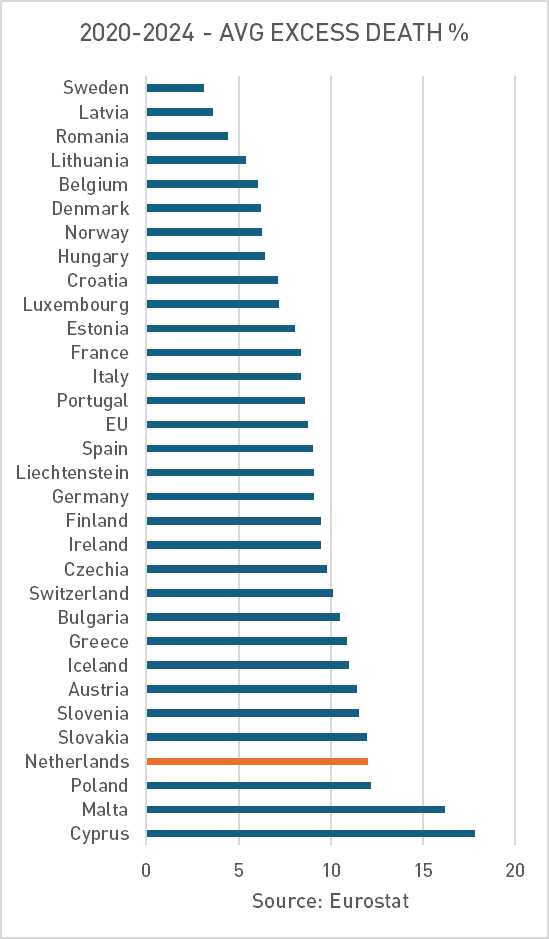
It is striking that both Malta and Cyprus will come out relatively much worse in 2024 than in 2023. Whatever the cause of the excess mortality, there could very well be an age-discriminatory effect.
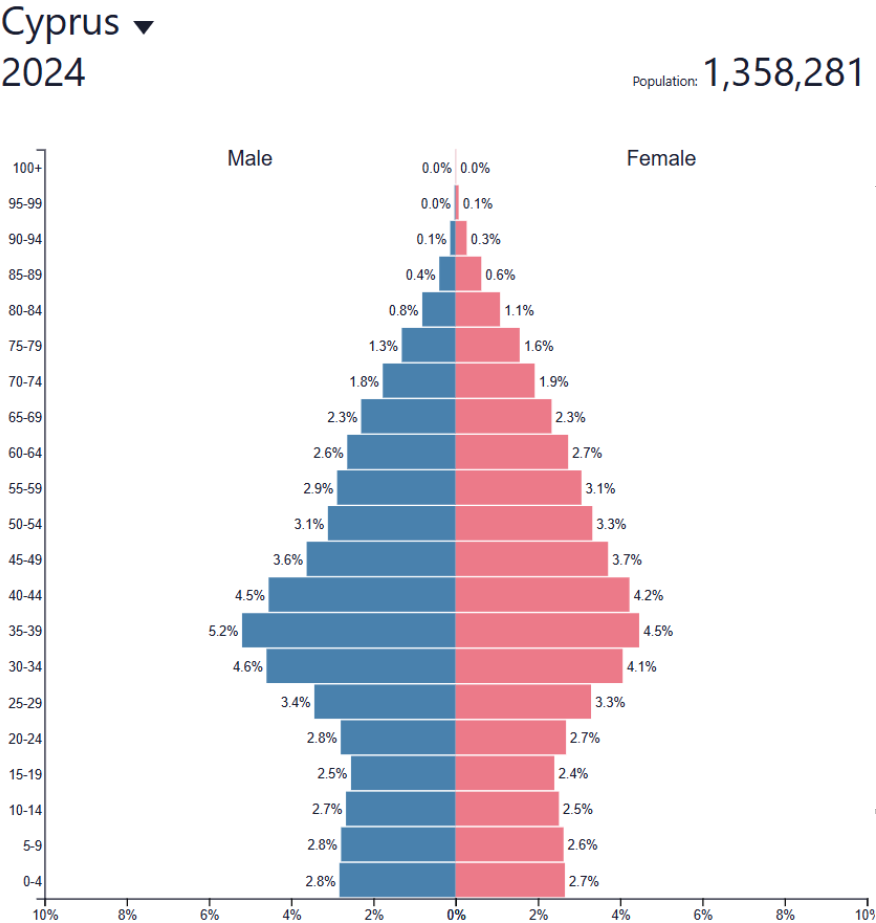
About misfits Malta and Cyprus
Malta and Cyprus are very small countries (540,000 and 1.35m inhabitants). This makes the uncertainties surrounding mortality slightly greater. More importantly: both Cyprus and Malta have very few inhabitants under the age of 30, see the pyramid. That pumps up mortality rates, because in those age categories, almost no one died, which would have brought the average down if they had had more of it. Now you can make that visible with an age correction (ASMR). Then the excess mortality will become less dramatic, because then you pretend that those countries have much more youth. But then again, they just don't have one. So ASMR does help explain it, but it does not reduce excess mortality.
England (UK) is also mentioned, but that is no longer recorded in Eurostat. England has had a hard time under corona. To say that they are really still doing so much worse than the Netherlands since then, that is a matter of opinion of Dr. van Gaalen. 8% to 10% excess mortality. It is a difference but don't forget that it should be about 0% for both countries! That is the norm that matters, not the ranking in Europe.
But that's how we know our elites, especially the more left-oriented ones. A little gaslighting and telling half-truths is not a crime, if you want to reassure the population, right...? As a leading intellectual you take responsibility and that means above all that you keep the people safe.
That's how Pieter Klok thinks about it too. (The recent interview with Ab Gietelink I haven't been able to watch out yet; I can't keep it up.)
The bridge with Fauci
Keeping the peace is - according to the people who know much better than we do - more important than being transparent and trying to get the truth out of the table. Lies and fabrications serve a higher purpose. That's how Fauci has justified his crimes. For himself that is. And one of his accomplices pardoned him, at least at the federal level. But each State can still initiate criminal prosecution independently. Let that party have started now. The Attorney-Generals of 17 states have put their heads together. That's what you get when you beat around the bush. Ruben, are you paying attention too?
Attorneys general of 17 US states join forces: Fauci on trial, Biden's pardon falls apart
February 10, 2025
Attorneys General of 17 U.S. states are joining forces to investigate Dr. Anthony Fauci's role in the response to the COVID-19 pandemic and his intentions to prosecute him at the state level, outside of the protection of his federal pardon.
Under the leadership of South Carolina Attorney General Alan Wilson, "the lawyers want to hold accountable for alleged mismanagement, misleading statements and suppression of scientific debate," according to a press release from Wilson's office.
Although Dr. Fauci's federal pardon protects him from prosecution at the national level, it does not protect him from charges or civil lawsuits at the state level. The coalition of attorneys has made clear they are prepared to prosecute Fauci if violations of state law are uncovered.
The attorneys general formalized their intentions in a letter to House Speaker Mike Johnson and Senate Majority Leader John Thune, asking for full cooperation in prosecuting violations of state law related to Dr. Fauci's pandemic management.
“President Biden's blanket pardon for Dr. Fauci is a shameful attempt to avoid accountability,” said PG Wilson. “If these findings indicate violations of state law, we are fully prepared to take appropriate action to ensure justice is served.”
The letter from the PGs follows the publication of the final report of the House Select Subcommittee on the Coronavirus Pandemic. The report details significant errors and possible misconduct by senior officials, including Dr. Fauci.
The subcommittee's report mentions Dr. Fauci's misleading public statements about the origins of COVID-19, mismanagement of funding by the National Institutes of Health (NIH), and attempts to suppress scientific debate about the risks of vaccines. Fauci has:
- the lab leak theory discredited despite supporting evidence,
- misled Congress about the gain-of-function research at the Wuhan Institute of Virology funded by the NIH,
- overseen the NIH's mismanagement of taxpayer funds earmarked for the EcoHealth Alliance,
- suppresses scientific criticism regarding the safety of vaccines.
"Despite these findings, former President Joe Biden granted a broad pardon request to Dr. Fauci, exempting him from federal prosecution for any offenses he committed during his tenure," the press release said. "However, the attorneys general insist that this federal pardon does not preclude legal action at the state level."
You can read the full letter here.
The coalition has formally asked Congress to release all relevant findings from federal investigations that "could lead to investigations and potential prosecutions at the state level."
This unprecedented move underscores the growing calls for accountability in the wake of the pandemic and signals that, pardon or not, the legal probe into Dr. Fauci is far from over.
The Dutch version of the letter You can read about it here (The EN original is on pages 9-16)
Signatories letter:

Who gets the popcorn?

Thanks for the info 🙂
Tribunals! I can't wait.
Thanks again, Anton!
It all remains bizarre. Suppose the "vaccinations" or those who promote them had to appear in court and evidence is presented by the prosecution that they have done more harm than good.
The graphs above are indirect evidence that something is going on, but causation has not been demonstrated. The main reason that causal relationship has not been demonstrated is that it has never been investigated, so then you don't find out. If you don't shoot, you don't score. Moreover, there is not really another suspect. More people falling, the aging population? All guesswork, and also demonstrably nonsense. Moreover, it is very worrying that the extra deaths partly occur in younger age groups.
Another aspect that leads to the suspect 'vaccines' is the composition of the injections. Not only has it been proven that the LNPs go through the entire body, but there is also evidence that the injections can be contaminated with DNA, leftovers from the mass production process. Spike proteins that are produced by the mRNA by the own cells have been proven to be demonstrated up to six months after injection. Autopsies on sudden deaths have shown inflammation caused by the same proteins.
There are countries where vaccination victims are compensated, or worse, the relatives of vaccination victims are compensated. So there are side effects, serious side effects even. So serious that people die from it.
The defense then puts forward the argument that the side effects are 'very rare', and that the 'vaccines' have saved millions of lives. They don't get much further. An honest judge would then ask 2 questions:
1. What is the definition of 'very rare', and at what value does the risk become unacceptable? I haven't seen that question answered anywhere. The Pfizer papers showed 1 in 800, an absurdly high score (Serious side effects, no swollen spot that disappears after a day).
2. How has it been determined that millions of lives have been saved? How can you determine what would happen if you had not carried out a certain action (vaccine rollout)? The only way would be to compare a large control group of unvaccinated people with a corresponding vaccinated control group. That did not happen, because the necessary data is not available. The unvaccinated people in the Pfizer trial were later vaccinated for 'humanitarian' reasons. What remains is based on models. Models who were actually always wrong during the 'crisis'. Not a very strong argument.
Then it is also true that the 'vaccines' do not actually prevent transmission. In fact, people who are 'vaccinated' appear to have flu-like symptoms more often than unvaccinated people.
Of course, there is much more to say about it. But after the above considerations, a little judge would decide to stop the rollout until it is clear that the injections have been proven to be 'safe and effective'?
The fact that we are still muddling through probably says enough. Every attempt at real insight is trained. Keeping the peace, indeed.
Had to get it off my chest again
I can still believe that there was a positive balance above 70 or 80 (delta variant). But if we accept that the risk there is 10,000 times greater than with young people, anyone with common sense understands that they should never give it under a certain age and forced.
It's yellow simple. At the beginning of 2020, covid was at most twice as severe as the regular flu. But due to built-up immunity in 2020 and early 2021, covid had become an average flu. So healthy people under sixty should never have been vaccinated. Especially not with an as yet approved vaccine that was based on the Wuhan variant that had not been around for a year in May 2021.
Good piece again Anton.
I am curious about the sequel in America. Whether there are judges who dare to take up the gauntlet: they are not small guys who run things behind the scenes.
Finally: not a word about all this in our MSM.
But yes, you say it yourself: keep the peace above all else.
Strange that this now mainly comes from the left.
To see the level of (excess) mortality in Malta etc in a better perspective, you can compare the (excess) mortality figures with, for example, the period 2016-2019.
You can use the later figures to see to what extent lockdowns have contributed to (excess) mortality. In Sweden clearly the least and also had the fewest lockdown measures. But I think the vaccination rate was just as high as or slightly higher than in the Netherlands.
I don't think there are many hard conclusions to be drawn, unfortunately.
And the protocols, general practitioners sidelined in case of flu-like complaints, ban on medicines. Strange things also happened in the hospitals. And why does van Gaalen mention New Zealand where, according to him, there is no excess mortality while there is excess mortality in the years of the shots. Everyone knows someone who feels the need to whisper something, but the decent people among us neatly adhere to the standards of decency, including me. In 2020 I learned that people in the msm media received considerable amounts of money for statements sent from politics and intelligence services. Of course with silence (strangle) contracts. Support the people who stick their necks out with donations! The breaking point feels near. The evil ones are also a little too fond of war in the hope that we will no longer have time to go after the past, it seems.
How do you determine excess mortality if you don't compare with previous periods and which better perspective do you mean?
We have already written a lot about Sweden: lucky with batches (see earlier article), or well primed with the real thing (the real virus had already circulated) before they were vaccinated. Assessing Tegnell, I also secretly wonder if everyone in Sweden who was already immune is still vaccinated. But yes, we just have to speculate in the hope of stumbling upon something.
I mean that the population composition in Cyprus etc for 2020 is probably similar to from 2020. If that is the case and it turns out that they were also at the top of excess mortality at the time and, for example, the Scandinavian countries at the bottom, then the figures are less useful to make a connection between excess mortality due to vaccinations or late hospital visits. In Sweden, I also think that more massive natural immunity and therefore 15 to 20 times better immunity than by the shots has resulted in less mortality. Perhaps most of them were therefore more resistant to the shots in 2022 etc.
Furthermore, in Scandinavia, selenium is actively added to products or in agricultural land to ensure that people do not become selenium deficient. Because a deficiency of it makes you much more susceptible to flu etc.
See also: relationship selenium deficiency and severe corona Ghent University.
Sorry Pjotr but if they were also 'at the top of excess mortality' as you call it in 2015-2019, for example, that level would not be excess mortality now.
I don't write that. I mean: 'If they were also (by far) at the top then'.
Then the composition of the population also played a significant role in that top position (by far) and therefore also after 2020.
That is why it is interesting to make that comparison to disprove or confirm a few things.
It's literally there...
But which comparison do you mean? Excess mortality is by definition ALWAYS a comparison with expected mortality and such an expectation is always based on the past. It is also adjusted if it deviates too long under normal circumstances.
It is impossible that Scandinavian countries have had undermortality for about 10 years. That there are countries with excess mortality for 10 years is also not possible. By definition not, under normal circumstances. By then, the expectation would have been adjusted a long time ago.
Forget Sweden for a moment, but you may be able to include the selenium effect and the naturally built up resistance due to infections in future articles about why Swedes suffered less from corona and/or the vaccinations.
You can only say something about changing (excess) mortality after 2020 if you have the figures from before 2020. So if Cyprus etc. had a low mortality rate, for example due to the absence of the severe flu in 2018, that may partly explain the (extra) high excess mortality after 2020.
This new excess mortality discussion will probably have to do with a report by Gijs van Loef that was recently published on New Year's Eve (see website https://gijsvanloef.nl/).
These are the main findings of that report:
Conclusions of international figures:
>The Netherlands has the largest excess mortality in Western Europe;
>The population of the Netherlands is ageing less than average ('less more elderly people');
>The Netherlands has a relatively low life expectancy;
>The remaining life expectancy among the elderly (65+/80+) is shorter in the Netherlands than elsewhere;
>The Netherlands had the lowest vaccination rate in '21;
Conclusions of the Netherlands specifically:
>Capacity shortages in healthcare are everywhere
>The labor shortage was 10% in '23;
>The labor shortage in (intensive) elderly care is possibly 12%;
>The largest excess mortality is among the most vulnerable 80+ people with a WLZ indication.
Van Loef is interested in the subject of excess mortality from a different angle. He sees excess mortality mainly as an important indicator of the system performance of health care.
However, the report is also interesting for critics of the corona crisis, such as us. That also provides (new) factual information.
The healthcare policy has certainly not helped. Unfortunately, he does not explain (or I missed it) how it suddenly changed in the second half of 2021 and is now getting better again painfully slowly. I think that's an important one.
I don't know if he can also demonstrate that pressure on healthcare can have this impact, it actually seems stiff to me. The vaccines, on the other hand, have been shown to be able to cause this mortality – but whether that is indeed the case we don't know...
The data that Gijs van Loef has collected from international sources regarding Excess mortality, I think that's right. However, he goes wrong in interpreting this data, especially with the effects of vaccination and the causes of excess mortality. For example, the indicator for average vaccination in 2021 and 2022 calculated by van Loef himself is nonsensical and misleading.
But I share his thesis that, for the explanation of excess mortality, we have to look at the special characteristics of our healthcare system. This is also directly justifiable from the collected figures, independent of the dubious analyses. The data from 14 Western European countries show:
1. There are 6 countries in Western Europe with the highest excess mortality in 2020;
2. There are 7 countries in Western Western Europe with the highest excess mortality in 2022;
3. In most group 1 countries, 2022 is the year with the second highest level;
4. In no group 2 country is 2020 the year with the second highest level.
Conclusion: 1-4 shows that 2022 is the crucial year for excess mortality internationally.
However, it is also apparent from the same data from Mr van Loef:
5. Excess mortality in the Netherlands cannot be classified in group 1 or 2. The variation over the 5 years in NL is very small. Actually the same picture with regard to the total mortality in the Netherlands, which is fairly stationary around 170K-171K in the period 2020-2024.
However, the Netherlands is the only odd one out among 14 countries. The very fact that the course of (excess) mortality in 2020-2024 in the Netherlands is both atypical in comparison with other countries and atypical in the own history of mortality in the Netherlands (just look at time series from the past) inevitably leads to the conclusion that:
6.Specific national system characteristics of the current health care system in the Netherlands must be included in the explanation of the excess mortality.
Q.E.D.
So there is a persistent high, almost stationary, excess mortality in healthcare in the Netherlands in 2020-2024 (seems like a '5-year plan'). In no other country in Western Europe does this situation occur. We have been the worst performing country, especially in recent years, because excess mortality remained high in Belgium and fell sharply elsewhere.
Gijs van Loef points to the acute shortage situations and market forces in healthcare as a possible explanation for the persistent poor performance of the Netherlands.
But is this correct? In Germany, there were no shortages but surpluses in healthcare, but there was still considerable excess mortality. At the moment they are working on reducing the overcapacity. Why wasn't massive work outsourced from the Netherlands to Germany during the COVID crisis, if shortages in NL were the problem?
Furthermore, it was precisely the 'market forces' in the Netherlands that were (partially) put out of action at the start of the COVID crisis by central control by the Ministry of Health, Welfare and Sport and the cabinet. Rather, misdirected market forces seem to be a problem: high mortality as a breach of contract is apparently insufficiently punished in the rates and budgeting of actors in healthcare. If the budgets of hospitals, nursing and care homes, general practices, and of course the budget of the Ministry of Health, Welfare and Sport had strongly negatively correlated with high mortality, would there have been such a high excess mortality in 2020-2024? Perhaps take a critical look at all those financing arrangements around death and COVID-19 in healthcare?
Those care capacity problems (if any, I don't see much of it) have nothing to do with, for example, the mortality among women between 40-50 years old and people in their sixties. And "inescapable" I don't know: we could also have just been unlucky with wrong batches in the beginning, broken or wrong cooling, whatever... See the article comparing batches (Sweden vs Denmark I think).
But of course, that care factor must also be included in the research. But then again, what research?
Everything that has been researched so far in terms of care explains less than 20% of the excess mortality – and then I estimate very broadly.