
Het is niet bij te houden wat er allemaal te lezen is. Hadden we in Nederland maar een krant met een redactie die een en ander kon schiften op kwaliteit en verhelderende duiding kon geven. Helaas - we moeten ons zelf een weg zien te banen door een menigte van roependen, jammerenden, onheil predikenden, elkaar besmuikt in het oor fluisterenden en schalks knipogenden. Haal daar maar eens de juiste informatie uit. En er is altijd wel een aanleiding voor een nieuw informatiebombardement. Op het moment zijn dat de 1) vaccinbijwerkingen, 2) de vaccinsamenleving en 3) de stijgende IC-opnames terwijl de overige parameters dalen. Eén voor een, de laatste met leestip.
1. Vaccine and thrombosis
We krijgen nu heel veel meldingen binnen over tromboseklachten na het vaccineren", zegt Lareb-directeur Kant. "Maar dat heeft te maken met de hoeveelheid aandacht die er nu voor is."
Agnes Kant, director of Lareb
So if attention is paid to reports of side effects, then that attention is actually the cause of the side effects ![]() . I certainly understand that there is a self-reinforcing factor in it.
. I certainly understand that there is a self-reinforcing factor in it.
Wetenschappers beweren zelfs dat het aantal trombosebijwerkingen LAGER was dan je zou verwachten op basis van normale statistieken. Een beter bewijs dat bijwerkingen ondergerapporteerd worden is er niet - het feit dat ze dat zelf niet zo opvatten vind ik beangstigend.
If you know that things should be reported but those reports don't come in, then you shouldn't be happy. Then you are like the oncologist who rejoices that so few women make appointments because of lumps in the breast. It just means that there is no reporting.
From Previous research at VAERS, the American Lareb dedicated to vaccine side effects, it was found that some side effects were reported in only a 1% of the cases. It concerns innocent or announced phenomena. The highest percentage was 68%.
Well, especially in the event of a death, you have other things on your mind than filling in forms on a website of a foundation whose name you may not even know. Just ask around in the private sphere: hardly anyone does that. Whether the doctor or general practitioner involved does it? Who knows.
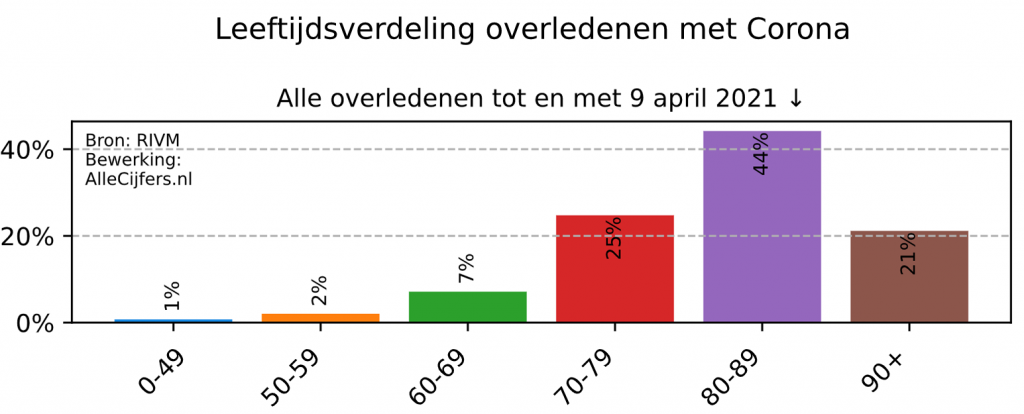
Een ander traject is het registreren van doodsoorzaken, ook al eerder behandeld. Artsen worden door de GGD's geïnstrueerd om als doodsoorzaak bij kwetsbare ouderen niet het vaccin in te vullen als doodsoorzaak. Het was immers het zwakke hart, de kanker of de hersenbloeding waardoor het tere gestel geen stress meer aankon. Vaccinatie dan is dan slechts "het laatste zetje" en wordt dus niet als bijwerking geregistreerd. Weinig huisartsen durven daarmee naar buiten te treden, Bart van Tienen was one.
Die coulante opstelling zie je gek genoeg nooit bij corona. Dat is nooit 'het laatste zetje' geweest, terwijl toch 90% van de covid-doden boven de 70 was.
So the link between those vaccines and thrombosis is still debatable, according to EMA, sometimes and sometimes not. And from all that attention you get a measurable condition like thrombosis, OK. Well, from the spike protein too:https://virusvaria.nl/het-verband-tussen-trombose-en.../(message from 3 weeks ago by the way. Go Click here directly to the research report.
Het klinkt ongeloofwaardig: als kwetsbare ouderen overlijden na vaccinatie dan is dat "het laatste zetje" en wordt dat niet als bijwerking geregistreerd. Testen ze daarentegen positief op corona, dan moeten ze wél als covid-dode worden gerekend, dat is géén laatste zetje. Je kunt immers niet voorzichtig genoeg zijn..."
2. Vaccine readiness is a driver
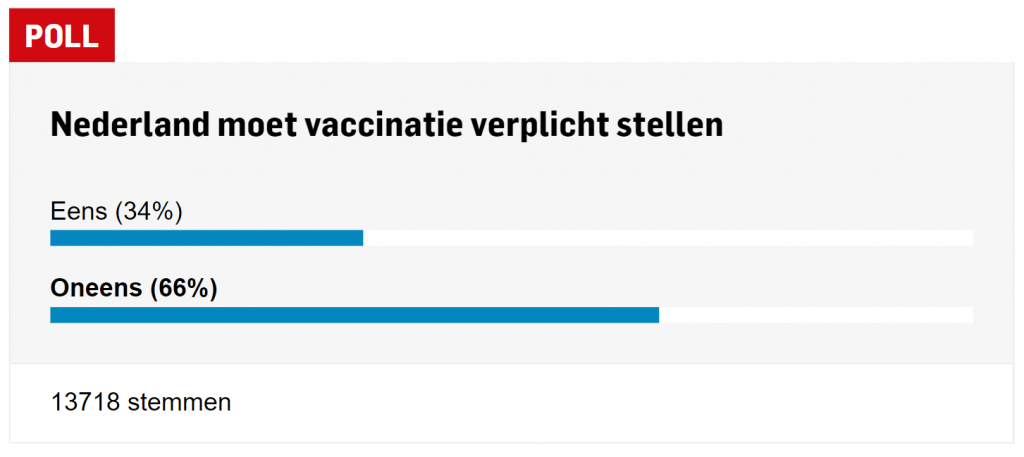
Het gaat niet zo goed met de vaccinbereidheid. Ik heb net (10 april, 's ochtends) onderstaande poll ingevuld bij De Gelderlander - met Oneens.
[erratum: I was pointed out by an extremely critical reader that your own willingness to vaccinate is different from your opinion on mandatory vaccination for everyone. If I then check the possible combinations:
- Agree with vaccination obligation, anti taking prophylactic mRNA therapy with immunizing effect
Het is inderdaad goed voorstelbaar dat mensen sterk VOOR vaccinatieplicht zijn omdat ze hem anders niet durven te nemen. Mensen zijn makkelijker voor vaccinatieplicht voor anderen als ze zelf denken een gegronde reden te hebben om de prik niet te hoeven nemen (je doet het niet voor jezelf, je doet het voor mij') - Disagree with vaccination obligation, pro taking prophylactic mRNA therapy with immunizing effect
You can be against the obligation while you want the vaccine yourself as soon as possible (so I have not sufficiently argued this) - Disagree and anti, Agree and pro
Tegen de plicht zijn en tegen de vaccinatie, of twee keer 'voor' behoeft hopelijk geen betoog. "Het is gezond, het zou verplicht moeten worden" of "Het is dodelijk, verplichten is genocide", kan allebei.
In the graph below, it may therefore be that a majority is against the obligation but is currently willing to be vaccinated themselves, although that seems a bit unlikely to me. The majority mainly think that vaccination only makes sense if everyone does it. I have no substantiation for this, other than that the majority is fine with it as long as the whole herd does it.. Thanks Max, for sharpening the sharpness. I have to be more careful with spontaneous last minute pamphlets.]
I think there should be differentiation. In the youngest age groups, the number of deaths after vaccination is in the same order of magnitude as when (perhaps) going through the disease, at least I haven't seen any other calculation yet. There are many reservations about the mRNA vaccinations, which I have listed in the article about the chicken vaccines by Marcel Levi
An age limit should actually be put on it: under 50 years of age you ARE not allowed to be vaccinated!
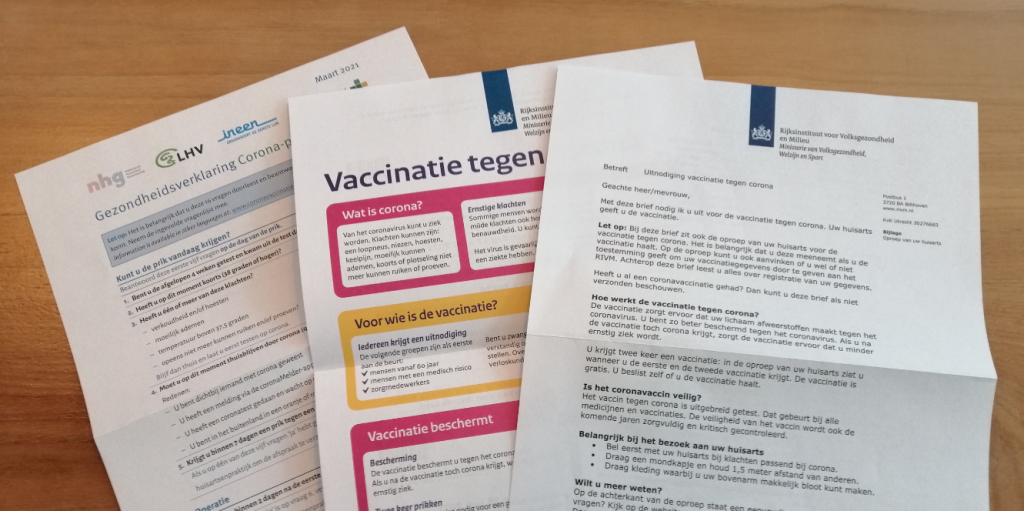
And then there is this in the bus.
Het uur van de waarheid. Nauwelijks boven de 60, zeer tegen verplichte vaccinatie, fel tegen v-paspoorten en een gesegregeerde testsamenleving, bezorgd over het beroerde voortraject van de vaccinaties en belangenverstrengelingen met machtige lobby's... Wist je trouwens dat de voorzitter van de EMA propagandiste is geweest van de efpia, de verenigde farmaceutenpromotor?). efpia is blij met haar carrière, ze heeft haar werk uitstekend gedaan bij de WHO en nu zit ze als voorzitter bij de EMA helemaal in een sleutelpositie. En inhoudelijk zitten ze goed op één lijn.
Voor een inbreker kan 'waakhondentrainer' een aardige bijverdienste zijn.
In response to the chairwoman of the EU medicines watchdog EMA (European Medicine Agency): Emer Crooke, educated and trained by the pharmaceutical lobby
Opgeroepen dus voor de strijd tegen het corona-monster. Beducht voor misinformatie van officiële zijde, ontevreden over de competentie van vaccinvoorstanders... Tja. Ik denk niet dat ik nu op de uitnodiging in ga, ik wacht nog even af. Heeft doktersadvies zin? Sommige van de artsen die ik tot nu toe heb gesproken moet ik bijpraten voordat ze er iets zinnigs over kunnen zeggen dus ik ben eigenlijk ook wel benieuwd naar het gesprek. Over naar het laatste onderwerp dat iedereen moet overhalen om op die uitnodiging in te gaan.
3. Fewer positives, fewer sick people, fewer deaths... More IC!
Eén van de blogs die ik met aandacht volg is dat van Jurjen Boorsma "STAY CALM AND STOP THE LOCKDOWN!". Hij post af en toe en alleen als hij weer inspiratie heeft gehad voor een goed doordacht en -uiteraard- onderbouwd artikel.
Ik was zelf ook bezig met het onderwerp dat veel coronisten in de ban houdt: "alle seinen staan op groen, maar op de IC's wordt de stormvlag gehesen". Jurjen zet in his latest blog article Several explanations in a row. You can skip my comment below, below is an updated version of it.
What struck me before, Jurjen also mentions:
“Ons is gevraagd ons maximaal in te spannen het aantal bedden uit te breiden en alle bedden te beleggen."
Arjen Hakbij, director of the Gelderse Vallei Hospital
Hospitals are therefore instructed by higher authorities to mobilize more ICU beds. Medium Care beds will become ICU beds. I understand that expansion, but how wise is it to immediately decree that that extra capacity must be filled immediately?
Without that filling of ICU beds, the ICU graphs will of course not go up. Admitting hopeless/underprivileged/too old sick people leads to longer treatment times, which is what you see happening. And suppose there really is a peak, what then? You don't have a place again! What kind of policy is that? Of course, a hospital wants to keep every bed billable. But if that turns out to be counterproductive, someone has to come up with something else. That's what we're voting for, isn't it?
Jurjen's article strengthened my idea of the cause of that ICU crowding. Alarming figures are urgently needed to boost vaccination readiness. After all, vaccination is the only way out. That is not malice, that is out of concern and feeling a responsibility to offer protection. Then only the ICU figures are still available.
Are there other options? We have infection, hospitalizations, ICU and mortality.
- Infections: The PCR test cycles have already been stepped up, runny children have already been drawn into the statistics, there is not much more to be gained from it.
- Admissions: de Jonge can hardly make more people sick on purpose, he certainly risks a scolding from the TK, if that comes true. Not good for career prospects.
- Mortality rates: Letting more people die is also a sensitive issue. And high mortality rates can work against you
- Dan blijft er maar één kengetal over: IC-opname. "We hebben meer mensen een kans gegeven, ten koste van alles."
Bijkomend voordeel is dat met het uitbreiden van IC-capaciteit niemand later iets te verwijten valt, het verweer ligt voor de hand: "Meer zorg, dat moest toch! Hoe kun je daarop tegen zijn? Er is al die tijd om geroepen om uitbreiding! En wat heeft uitbreiding voor zin als je er verder niks mee doet?" Geen speld tussen te krijgen voor de gemiddelde journalist.
Faith, distrust or disbelief
Het gaat niet om 'geloven in' het manipuleren van data. Die data kloppen heus wel maar het zij gezegd: ik geloof überhaupt niets (geloof ik, of ik moet wat vergeten 😉 ). Ik kijk echter wel naar de tot dusver gevolgde lijn en wat daar wel of niet in zou passen vanuit de onderliggende motivatie. Dat heb ik mij eigen gemaakt vanuit mijn professie. Dan zie ik dat tot nu alles uit de kast is getrokken om de angst erin te houden. Gedragsexperimenten worden zelfs toegestaan.
There is lying, manipulation and brainwashing. Major media conduct propaganda. Scientists talk gibberish. All this in good conscience of the clique that really, really, wants the very best for us.
At the same time as the alarm signals from the ICU, a very thick relaxation carrot is very emphatically held up. Where that suddenly comes from, no one knows. It seems like a strategy for behavioral change.
Who gets the cake, who gets the gard. And soon the cake will go back into the box because then we have been disobedient.

Ik zie weinig onverwachts in wat er gebeurt. Of het met 'geloven in het opdrijven van cijfers' te maken heeft? Ik geloof zeker niet in kwade intenties. "De mensen moeten begrijpen hoe ernstig het is en dat het niet weggaat als ze niet precies doen wat wij zeggen!". Dat "zeggen ze tegen elkaar", de OMT-ers. Radeloos zijn ze, hun maatregelen blijven maar slagen in de lucht omdat niemand ze goed opvolgt. Hoe breng je dat mensen toch in hemelsnaam aan het verstand... Dreigende toekomstbeelden en beloftes met beloningen!
I think there is a good chance that it happened that way and it is also in the line of -indeed- manipulations, but not specifically of figures.
The Machiavelli Prize was completely justified.
