
International comparisons
More and more articles are appearing that expose the harmful effects and ineffectiveness of vaccines. Usually these are clinical studies, describing harmful mechanisms. But how often do these actually occur? What about the bare figures, excess mortality and its relation to the number of vaccinations? A week ago, we wrote a article on the effectiveness of vaccination based on international figures. Even earlier, we presented a calculation model detailing the possible relationship between excess mortality and the number of vaccinations, which were put there.
This article is an in-depth look at last week's virus variety article, now also published on maurice.nl.:
We will now use the available information from 34 countries to deepen last week's exercise. Through the public figures from OurWorldInData we have compiled the death rates of 818 million inhabitants. This includes virtually all European countries plus Russia, Israel, Canada, Australia and South Africa.
We divided the corona time into three phases in order to draw conclusions about vaccine effectiveness. These were these phases, which we will briefly denote below using only the year:
- 2020: the period from April 2020 to March 2021. 12 months containing virtually no vaccinations, the "unvaccinated period". The excess mortality was largely caused by the first and second corona waves.
- 2021: the period from June 2021 to May 2022. Also 12 months in which almost everyone who had the basic series had actually been vaccinated. The "vaccinated period". Mortality patterns could be affected by vaccinations.
- 2022: the period from April to November 2022. The Omikron period, 8 months. The number of deaths from corona has fallen sharply and the picture is dominated by the “unexplained excess mortality” .
This way, we get 3 mortality figures for each country, one for each period, and we compare them with the average number of vaccines given per inhabitant of that country. Of course, there is still some difference, because it will make a difference whether one person had 5 shots or 5 people each had one shot. But for this analysis, we're just trying to recognize the big picture.
"Unvaccinated period"
There was no vaccination in 2020. We make a graph plotting the excess mortality in that year against the vaccines to be put in the future. You would expect that graph to show no relationship then, but it seems to show one:
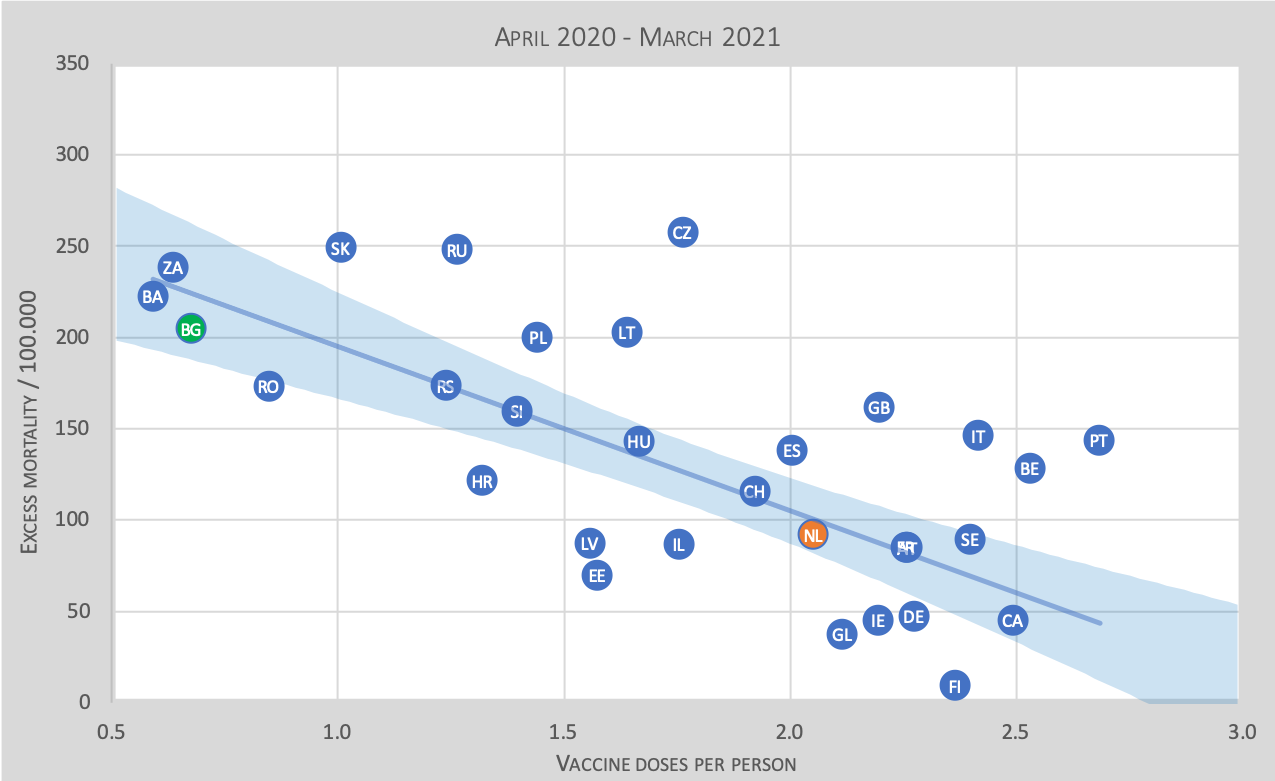
This graph shows the excess deaths per 100,000 population for each of the 34 countries. On the horizontal axis we read the average number of vaccinations given per capita as of 2021. On the vertical axis the excess deaths per 100,000 population.
Bulgaria is often cited as an example of a country where there was low vaccination coverage and high excess mortality to emphasize that vaccination is much needed. So we are going to follow that country and give it a green bullet in the graph. The Netherlands we put in with an orange bullet.
We read in the graph that in Bulgaria there is an excess mortality of over 200 people at an average of 0.7 vaccinations per person. For comparison, we look at the Netherlands (orange dot), where the excess mortality was only 95 in 2020 at 2.05 vaccinations per person. So if you look superficially you would think that vaccinations have had a very beneficial impact here.
But.... these are vaccinations yet to be put! Thus, these could not possibly have influenced the mortality in 2020. So the link between this excess mortality and future vaccination must be an indirect one. The fact that all the countries with the combination of high excess mortality in 2020 and low vaccination coverage in 2021 are all located in Eastern Europe seems to give a clue. Could it be the (quality of) health care? It is an interesting observation in itself, but we leave it to others to find a conclusive explanation for this. We will now look at the same figures for 2021.
"The vaccinated period"
From January to June 2021, vaccination was carried out with the baseline series. Especially in April and May, it is unclear whether a death should be attributed to the unvaccinated period or to the vaccinated period anyway. Therefore, as indicated, we omit this period and start in June 2021.
We were promised a protection of possibly even more than 95%, so we should then see that reflected as lower excess mortality rates in an identical graph to the 2020 one. This is this graph:
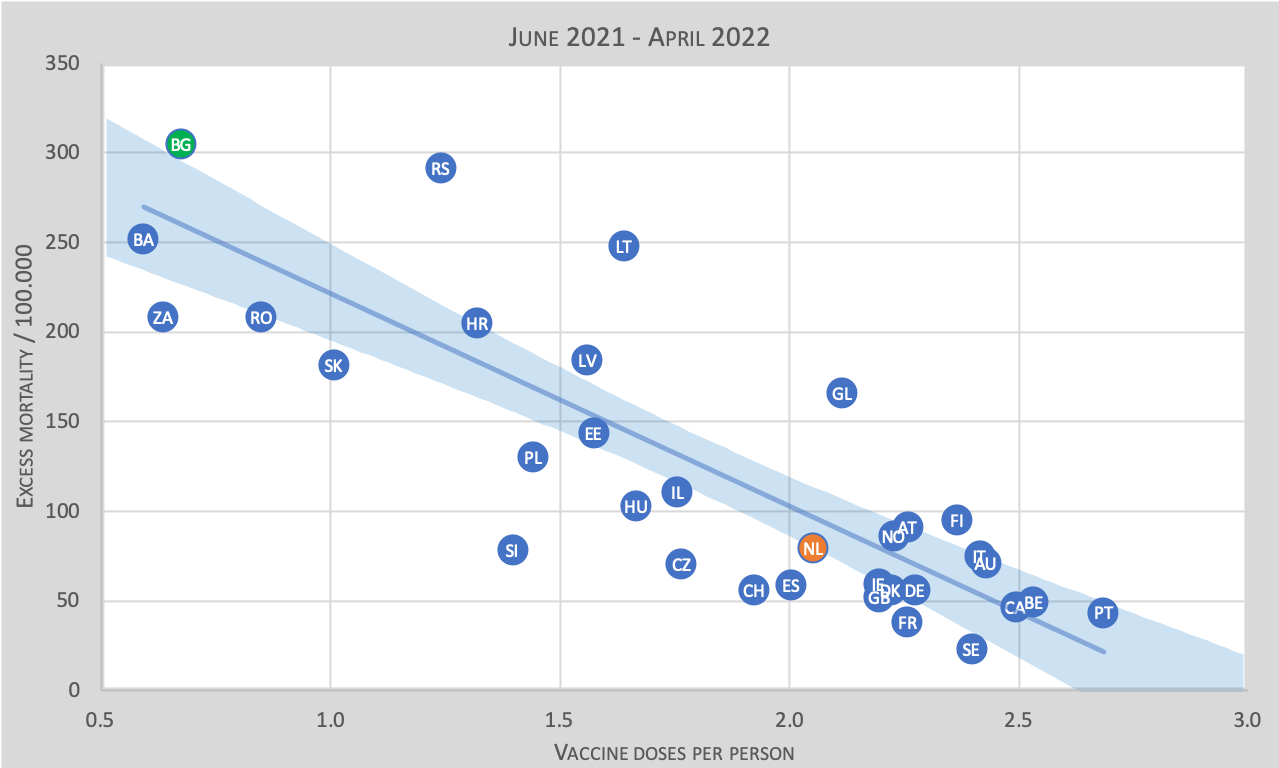
Appearing to be the same graph as the 2020 graph, the differences are very minimal. Even so small that there is no significant difference between the two lines from the two graphs. So actually, on average, we see barely any difference between pre- and post-vaccination excess mortality.
Now it is said that "without vaccination there would have been many more people who would have died....". RIVM has explicitly stated that thanks to the vaccination 88,000 hospitalizations would have been prevented between 2 August 2021 and 30 August 2022. But if that were true, there should have been a huge increase in admissions and thus in excess mortality in the little-vaccinated countries. But there is no evidence of that at all! The proportions of excess deaths in both high and low vaccinated countries in those two graphs remained the same on average. From that one might then conclude that vaccination has not played a significant factor in reducing mortality.
'The Omikron period'
In the third year, Omikron was the variant that displaced Delta. In February, Omikron was dominant and there was also a flu wave for the first time again in March. Therefore, we let the third period begin just after this (in April), to include only the (occurrence of) death from Omikron. Also, starting in April, the “unexplained excess mortality” clearly visible. It was numerically demonstrable before, but hid behind the corona waves each time.
In our article Excess mortality across the border we have already quantified this excess mortality. A short- and long-term probability was presented there. Based on these probabilities, our mathematical model predicted a mortality of 63/100,000, given the vaccination pattern in the Netherlands.
Let's look at the chart and see if we find that:
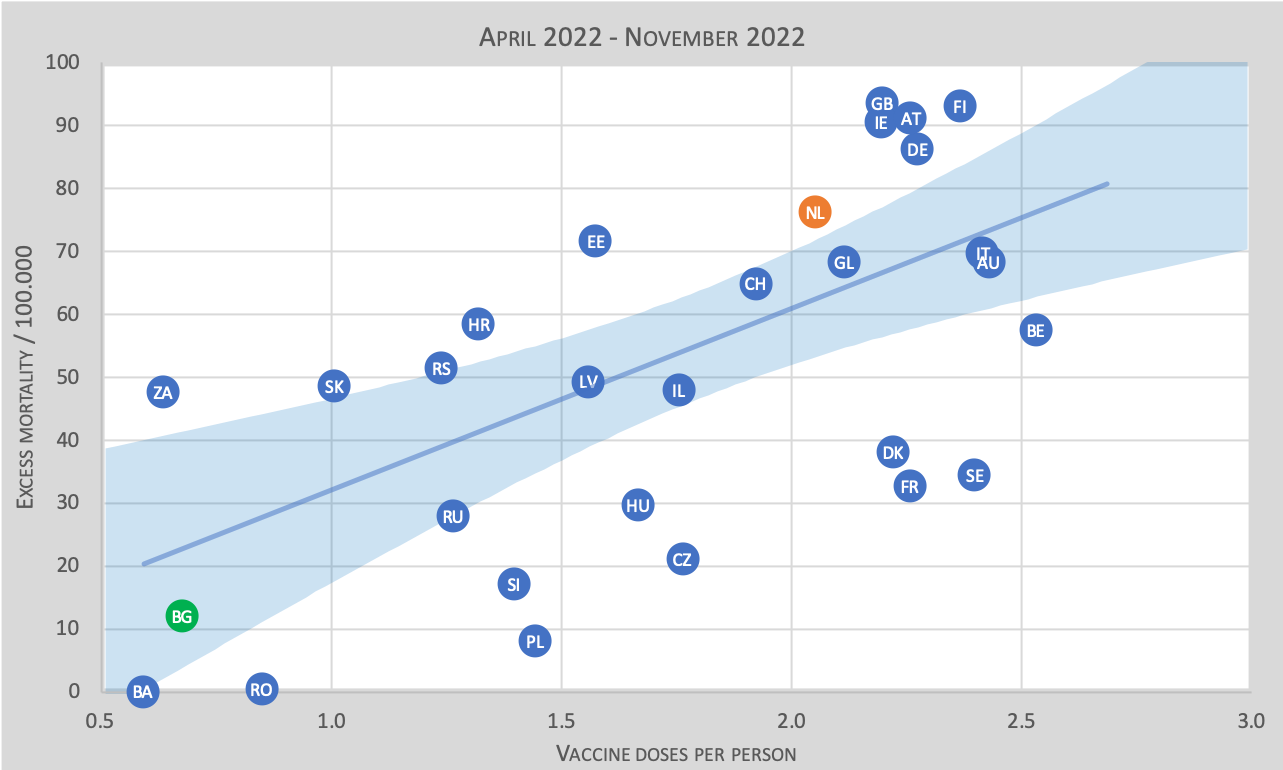
Now suddenly we see a completely different picture than in 2020 and 2021. On average, excess mortality now increases linearly with the number of vaccines given! In fact, the regression line runs almost through zero, from which one could conclude that without vaccination there would have been no excess mortality.
Bulgaria is now suddenly the best boy in the class! The excess mortality there is only 12/100,000 at 0.7 vaccines p.p. while in the Netherlands, for example, it is already 76 with three times as many vaccinated.
Summary
Now that we have calculated the regression lines for these three periods, we can summarize them in a table and draw conclusions. We define three notional groups of countries, with different vaccination rates: High (2.5 p.p.), Low (0,5 p.p.) and Unvaccinated. The latter group in particular, of course, is a truly fictitious one, since you cannot find a country in Europe that has not been vaccinated, but you can "read" the regression line at a value of 0 p.p.
Each graph also shows the uncertainty as a light blue bandwidth. We use these to determine the lower and upper limits.
We have three periods, so for each of those periods we can now estimate how many excess deaths per 100,000 there will be at the given vaccination rate. We can also calculate a reliability (p=0.1) with the lower and upper limits in parentheses. This is then this table:
| High | Low | Unvaccinated | |
| 2020 | 60 (34 – 87) | 218 (183 – 254) | 285 (230 – 340) |
| 2021 | 44 (19 – 68) | 252 (220 – 285) | 340 (289 – 391) |
| 2022 | 75 (62 – 89) | 25 (7 – 42) | 3 (-24 – 31) |
We see that while there is a small difference between 2020 and 2021, the areas of uncertainty overlap and there is no significant difference between these years. Thus, on average, vaccination did not significantly reduce or increase excess mortality in 2021.
If we look at 2022, we see that for the highly vaccinated group there is actually no difference from previous years either: the same number of deaths, while we know from other sources that deaths from Corona itself (=Omikron) have become very low. In the Netherlands a total of 2600 deaths from corona, or 15 per 100,000 (out of a total of 76 per 100,000). So here we are faced with the unexplained excess mortality!
Among low-vaccinated countries, the excess mortality has become very low: 25/100,000 and that includes corona.
The last thing the regression line seems to be telling us is that the risk is 1:3000, to be during these 8 months to die from one vaccination. That is still on the basis of 818 million inhabitants. Of course, there could be another causality, but it will first have to be explicitly identified as a candidate and also apply to the other 33 countries in this study.
There is still no decline in unexplained excess mortality so this 1:3000 will certainly continue to increase. In our article Vaccinations modeled we calculated that the ultimate risk could be around 1:1000, if we include all figures since the first vaccination.
Conclusions
Simply pointing to a country like Bulgaria, where there was little vaccination with a very high excess mortality in 2021, as a resounding example that vaccination was very successful, actually turns out to be nonsense when the 2020 graph is also looked at and the 2022 graph. Because in 2020 Bulgaria also had higher excess mortality than most other countries and in 2022 Bulgaria had one of the lowest excess mortality rates.
In addition, on average, we see that in these 34 countries, vaccination did not reduce excess mortality. In absolute terms this could be explained by the virus becoming more aggressive. But then you should have seen a sharp increase in this excess mortality in low-vaccinated countries. And we did not see that either, the excess mortality in 2021 remained almost the same there as in 2020.
These numerical findings are not yet conclusive proof of vaccinations not working properly, but should at least prompt the government to commission serious research into this before proceeding with boosting.
Questions
Following these conclusions, the government in particular, sitting in the doctor's chair, should ask itself some questions:
- How is it that mass vaccination did not reduce excess mortality?
- Why do countries that have barely vaccinated now have by far the lowest excess mortality?
- Why do countries with minimal vaccination now have no deaths from corona anyway?
- Why does the excess mortality among the highly vaccinated countries seem to continue to increase rather than decrease?
- Why do we not see an increase in excess mortality in the lowly vaccinated countries if 88,000 hospital admissions would have been prevented in the Netherlands thanks to vaccination?
The answers to these questions could help make better decisions in later epidemics.
Discussion: it's because of the Eastern European countries
Within our group of corona watchers, opinions are divided on the latest chart. Below is a brief reflection of our thoughts.
It is notable that the countries with the lowest excess mortality in 2022 and the lowest vaccination coverage have more in common: it is a cluster of Eastern European countries. This strongly influences the course of the trend line, it was thought. It also raises the question of whether other factors are not at play with those countries: geographic location, political system, level of health care, diet, health status of the population or life expectancy, to name a few.
Many of these demographics are already factored into the normal baseline mortality of those countries, so this should not be recognizable in the excess mortality.
The hypothesis was also suggested that the lower excess mortality in 2022 in those countries could be a result of the high mortality in 2020 and 2021. On the other hand, this 'under-mortality effect' was not visible in 2021, compared to 2020. Then in 2020 it should have been the turn of the first half of the vulnerable population in all those countries and in 2021 exactly the other half (not half of that). In 2022, the reservoir of vulnerable people will have become exactly so small that they will end up in the lowest regions. It's a possibility.
This becomes especially complicated because the data are not there to support this statement. It is of course conceivable - but so are more scenarios. For now, the great common denominator remains vaccination rates.
Oursimple linear modelwhich calculates additional mortality based on the number of vaccination doses, is grafted onto developments in the Netherlands and tested against the figures of 30 other countries (see earlierarticle). The Eastern European countries also fitted well within that line.
Surely we put it to the test: will the connection indeed be lost as soon as those Eastern European countries are omitted from the equation, as that Eastern bloc cluster suggests? We can see in the graph below what happens then: the uncertainty margins for the low numbers of vaccinations become much larger. That goes without saying, because if we only select countries with a (virtually) equal vaccination coverage, the differences between different vaccination rates become less clear. Any value of the regression line within the blue uncertainty area is possible and the model's forecast (indicated by the orange line) is still well within these uncertainty margins.
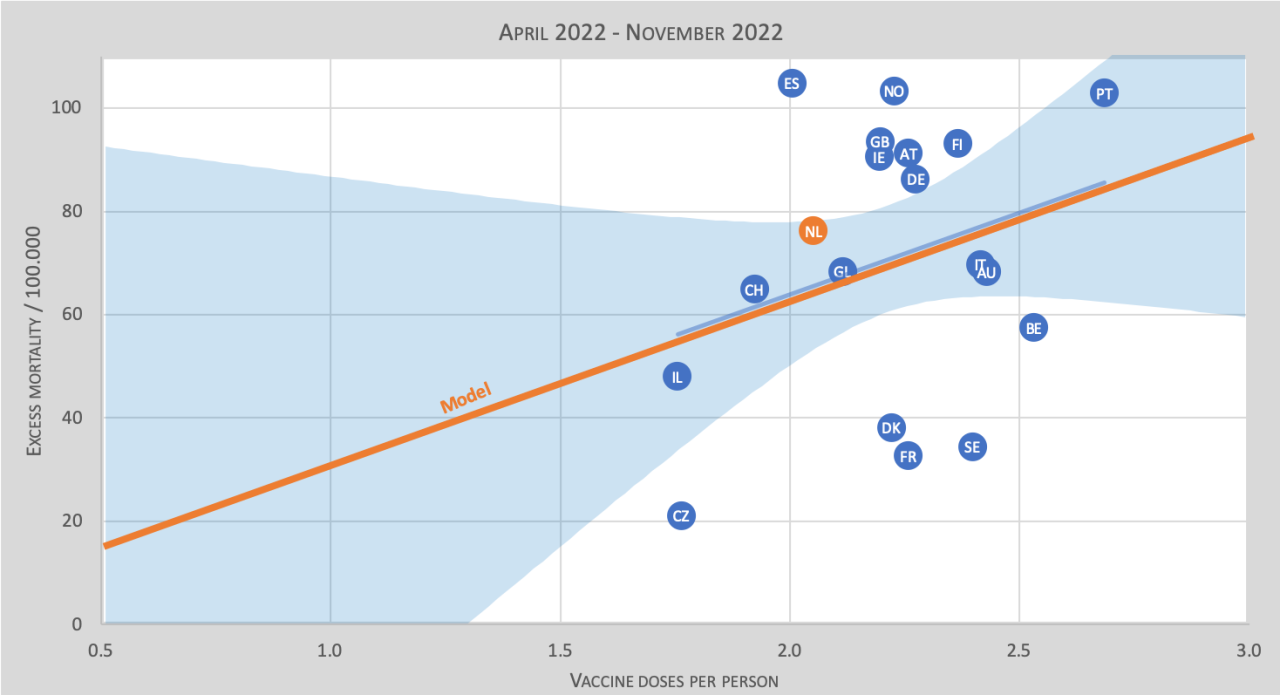
That thecalculatedregression line is rising, so actually says little. Only the average value in the middle of the point cloud has any value: 55-80, almost the same as if we include all countries and also perfectly matching our calculation model. Let us also not forget that we are talking about the summer period in Europe: the months in which we should not see excess mortality at all! Let alone in all European countries.
Anton, I have to say something. Nice approach, and must have taken a lot of time. Maybe some additional ideas that eg. Scandinavia better explain. One difference that you have not taken into account is the 'vaccine' variation. From sometime in 2022, the bivalent vaccines will have been introduced. They have been tested even less than the original injections. How the immune system reacts to it, no one knows.
In addition, in a number of countries people have stopped pricking (under 50 or 60). In our cool country, the are still recommended through propaganda. So total number of jabs in, for example, Sweden can be quite high, but how recent are those jab rounds? And with what type of vaccine? It doesn't make the comparison any easier, I realize that. Aspirating can also have an impact (Denmark).
I'm not saying for sure that it has an impact, but it is certainly a big uncertainty that could be relevant.
Dear Cees,
You're absolutely right, of course. There is a lot more to the research and quantification. Actually, this should be a suggestion to our Minister of Health, Ernst Kuipers, but he has actually ruled out vaccination in advance as a possible cause of excess mortality. A very first step is to come up with clear, "simple" figures, which will hopefully open the door to the willingness to look at this. If that happens, then we have achieved our goal. What's next.... that in turn smacks of something international. We do not get beyond the data that IS available.
The graphs in this article show that there is a substantial bandwidth between countries. Countries with the same vaccination coverage can still have very different excess mortality. This can indeed be due to vaccine variation and also differences in periods in which the vaccines are put. Another factor may be the production variation in vaccines. The registration of side effects in Vaers shows that the reporting of side effects is very irregularly distributed over the production batches. Some batches show many more side effects than others. In itself, this is a reason to reconsider mass vaccination. But let's avoid jumping to conclusions: in addition to vaccination, there may still be very different reasons for excess mortality.
Thank you, Herman. It's not clear to me how to respond to your thread, so it might end up in a strange place.
The number of variables is indeed overwhelming. Just saw on joel smalley's site a nice analysis of New South Wales, Australia. Looks like they created the perfect storm there. First isolate everyone for a long time so that the immune systems get much less stimuli than usual. Then fill everyone with mRNA vaccines so that immune systems are 'primed' for a virus that no longer exists. The relatively harmless omicron can then suddenly turn into a deadly virus? And the common flu also hits much harder. Just like here in the Netherlands (the flu situation. Doctors wonder why the flu lasts more seriously and longer than usual). In my opinion, exactly what Geert vd Bossche has been warning about for a long time and what he has been ridiculed for.
Those excess mortality values of Bulgaria and South Africa and BA (?) are minimized in 2022. I can only explain that because in 2020 and 2021 the corona variant was more deadly, and in 2022 innocent, while the health or health care in those countries is less? How else can you explain it if vaccination plays no or almost no role? But hey, the vertical scale of 2021 runs to 350, that of 2020 and 2022 to 100! Mmmm. Hard to compare. If I compare a little, there are only a few countries that have more excess mortality,
GB, DE and IE. (CH, be ietjes hoger, some countries are not in both graphs). The rest or equal or less. NL the same. You can apparently better conclude that .....?? That poorer countries are more vulnerable to aggressive viruses, that richer countries are less vulnerable, and that multiple vaccinations do little to help the richer countries or sometimes work against them in the long run? The poorer countries might score well in 2022 because the vulnerable have already died? You should add 2019, then you can draw better conclusions. It remains necessary to compare the figures between ages and the number of vaccinations in 1 country. I have already read that in the UK vaccinations helped a lot with the first wave and then no longer, even for certain age categories you became more vulnerable because of the vaccinations. Do I still get it? By the way, I am 63, not vaccinated, 2x sick but not very much, the first time a bit sicker, and the chance I die at all this year, I have looked up, is 1% approximately. In short, there are worse problems.
Dear French,
2019 is already indirectly in it, because this is about excess mortality. This is always relative to the baseline and is in principle based on a 5-year average, adjusted for epidemic waves. CBS apparently has a clever way to do this, because the baseline for 2022 has been increased by only 0.5% compared to 2021. Corona has (rightly) not increased it much.
And yes, there are differences, partly unexplained. But if the vaccines had really protected us, you should have seen big differences. 10X as low mortality or something. And in 2022, under-mortality after so many excess deaths. Nothing at all, the opposite in the highly vaccinated countries
First of all, kudos for yet another beautiful piece of work. Thanks Herman and Anton. As soon as I receive a notification of a new article on Virusvaria, I drop everything out of my hands and I will read it immediately.
I would like to say something about the great similarity of the periods 2020 and 2021. The virus variants in 2021 were less pathogenic than in 2020. Apart from that, by building up natural immunity in 2020 and 'microvaccination' (as Maurice de Hond calls it based on work by Prof. Bouma), you can expect that the excess mortality due to corona will decrease in 2021 (compared to 2020). Especially if you also expect a bit of under-mortality due to the events in 2020. That this did not happen is strange.
If you assume that vaccination is indeed the (main) cause of excess mortality in 2022, then this has already played a role in your period of 2021. If you were to correct for the harmful effects of the vaccination in 2021, and remove excess mortality from vaccination, then the regression line should become steeper in 2021 (fall more sharply). Ergo, there will be a difference with 2020: the vaccinations will have therefore provided an advantage in the short term. Your period 2021 is too long (until April 2022) to see that. You may have lost significance due to the choice of periods. And so vaccinations may have an advantage in the short term, but in the longer term they are only harmful. And no one knows for how long.
Definitely a good point Henk. We have only looked at the net total result here. In the end, All-Cause-Mortality is the ultimate test. With detailed data on vaccination statuses and causes of death, you could pull everything apart much better.
"Yes, the Covid vaccines can cause myocarditis and pericarditis. And yes, people (older and younger) die from the vaccines as a result. But... the vaccines have saved tens of thousands of lives. So feel free to take the new booster. The advantages (still) outweigh the disadvantages".
According to The Telegraph's Maarten Keulemans: https://12ft.io/proxy?q=https%3A%2F%2Fwww.telegraph.co.uk%2Fhealth-fitness%2Fbody%2Fcritics-claim-covid-jabs-causing-heart-problems-do-have-proof%2F
Dear Anton, I only see this article now. Broadly speaking, it seems to me to be very good and important. Still, I noticed a few things, one even in bold:
1. "But if that were true, then there should have been a huge increase in admissions and therefore in excess mortality in the few vaccinated countries."
But it is not to be expected that not vaccinating will result in an increase in excess mortality with a variant of the disease that is at most as strong!
I would say: "But if that were true, then there should have been a huge drop in admissions and therefore in excess mortality in the many vaccinated countries."
This is also stated lower in the article: "on average, vaccination has not reduced excess mortality in these 34 countries."
The first question at the end of the article is also in line with this. But the last question is the wrong way around.
2. The conclusion just below "But if that would be true" doesn't sit well with me either:
"From that, you could conclude that vaccination did not play a significant factor in reducing mortality."
But according to the graphs, mortality in the Netherlands had hardly decreased and internationally there was little or no reduction. Maybe better:
"From that, you could conclude that vaccination has not reduced mortality, if at all."
Fortunately, none of this makes much difference to the overall consideration. I really appreciate those articles, thanks again!
PS. another point:
– "Many of these demographics have already been factored into the normal baseline mortality of those countries, so that should not be recognizable in the excess mortality."
I have my doubts about that. The normal baseline mortality rate can be higher or lower, without saying anything about how well a population group is able to cope with a new virus.
Thanks for your comment.
1. You write: "it is not to be expected that not vaccinating will result in an increase in excess mortality".
That is the line of thought if you want to use such a graph to show that vaccination helps. Otherwise, vaccination would be pointless anyway and that would make this whole discussion superfluous.
2. Doesn't really matter, it's more of a semantic discussion without much impact on the basic idea.
PS. another point:
– "A lot of the demographics have already been discounted... Without that saying anything about how well a population group is able to cope with a new virus." That's right, of course, that's why I write "A lot of". What remains cannot explain such figures. That demographic does include the age structure, which is a very important predictor.
Maybe I didn't make it clear enough, sorry.
No change of action in a stable situation has the expected effect of no change, and certainly not a huge increase in excess mortality.
Vaccination is intended to reduce excess mortality; Continuing not to vaccinate in the event of an almost constant pandemic has the expected consequence that pandemic-caused excess mortality will remain more or less constant – not that it will increase sharply.