
Last week, Robert F. Kennedy cited a study by a Danish research group. According to fact-checkers, RFK thrives by the grace of Conspiracy theories. All the nicer if the principal investigator himself gets involved in the dispute. Christine Stabell Benn has already stood out for her down-to-earth and realistic view of her own field of work: vaccinations. She speaks like a scientist, which is of a different order than the talk show pundits and civil servants who peddle the products of American high earners in our country. Below is the extremely readable contribution on LinkedIn (On Robert F Kennedy Jr's comments on our studies of diphtheria-tetanus-pertussis vaccine), translated into Dutch.
Zij vat de kernpunten van het artikel van RFK zelf als volgt samen: "zeer in het kort kloppen sommige details niet: We zijn niet door de Deense overheid op pad gestuurd om DTP-vaccin te bestuderen; Bill Gates is er niet bij betrokken en we hebben niet slechts één onderzoek gedaan op basis van 30 jaar gegevens, maar vele onderzoeken over een periode van 30 jaar. De belangrijkste boodschap - dat we een ernstig veiligheidssignaal hebben ontdekt met betrekking tot DTP-vaccin voor vrouwen - is echter correct."
On what Robert F Kennedy Jr. said about our research on the diphtheria-tetanus-pertussis vaccine
© Christine Stabell Benn
Professor of World Health @SDU. We study the general health effects of vaccines in Guinea-Bissau and Denmark and find that they have important nonspecific effects #NSEvac
18 July 2023
Many people have alerted me to the fact that Robert F Kennedy Jr. mentioned our group's studies on the whole-cell diphtheria-tetanus-pertussis (DTP) vaccine [Note: the P stands for Pertussis = Whooping Cough, not Polio] which is used in Africa. They asked me if the story is true. Allow me to present the story from our perspective. In short, some of the details are wrong, but the overall message - that we have discovered a serious safety signal regarding the DTP vaccine for women - is correct.
Our research group, the Bandim Health Project (BHP), is opgericht in 1978. Het is geen overheidsgroep. Afgezien van de afgelopen vijf jaar, waarin we een beetje basisfinanciering hebben ontvangen van onze nieuwe "gastheer", de Deense State University of Southern Denmark, we are only funded by grants for specific research projects. We apply for these grants from public and private foundations. The funders have no role in the investigations. So we are an independent research group with no conflicts of interest.
BHP has a field station in Guinea-Bissau in Africa. Here, infant mortality has traditionally been extremely high, almost exclusively due to infectious diseases. In the eighties, the founder of BHP discovered, Prof. Peter Aaby, that a measles vaccine reduced infant mortality much more sharply dan te verklaren was door de preventie van mazeleninfectie. Het bleek dat het mazelenvaccin gunstige "niet-specifieke effecten" (NSE's), which strengthened the immune system and lowered the risk of dying from infections in general.
This led to an investigation of all childhood vaccines. Most people did not know that the childhood vaccines had never been studied for their effects on other infections, only on the target infection(s). We found that all the vaccines we examined had NSEs.
A pattern emerged. All live vaccines we examined had favorable NSEs. However, with the DTP vaccine, a non-live vaccine, we consistently found that the vaccine was associated with negative NSEs, especially in girls. So despite being protected against three fatal diseases, girls who received DTP vaccine had a higher risk of dying than girls who did not receive DTP vaccine, and DTP-vaccinated girls had a higher risk of dying than DTP-vaccinated boys, even though the opposite was true after live vaccines.
With this worrying safety signal, we went to the WHO. Initially, the WHO commissioned a number of other sites to test our findings. These studies came out with extremely positive effects of DTP vaccine. However, they had used a flawed methodology, something that was recognized in 2006 and the WHO did state that they "het bewijs van niet-specifieke effecten van vaccinatie in de gaten zouden houden".
Studies showing nonspecific effects of vaccines continued to pile up, and in 2013, WHO's Strategic Advisory Group of Experts on Immunization (SAGE) set up a working group on the non-specific effects of vaccines and conducted a review of the NSEs of the live measles and BCG vaccines and the non-live DTP vaccine. The review was published in 2016 Bmj. In totaal werden 10 DTP-onderzoeken opgenomen in de analyse. Terwijl werd waargenomen dat de twee levende vaccins de algehele sterfte veel meer verminderden dan werd verklaard door de preventie van de doelziekten, was het tegenovergestelde het geval voor het DTP-vaccin, waarvoor de reviewers concludeerden dat "Reception of DTP (almost always at the same time with orally administered polio vaccine) was associated with possible increases in all-cause mortality on average (relative risk 1.38, 0.92 to 2.08) from 10 studies with a high risk of bias; This effect seemed to be stronger in girls than in boys".
Het ontvangen van mazelenvaccin of BCG-vaccin met of na DTP-vaccin werd geassocieerd met een lagere mortaliteit dan wanneer DTP het meest recente vaccin was. De beoordelaars adviseerden dat het bewijs "indicates the need for randomised trials to investigate the place of DTP in the vaccination schedule".

Following their meeting in April 2014, the WHO SAGE instructed the IVIR-AC Commission to define research questions related to NSEs should be investigated. However, there are apparently no studies planned regarding DTP, now almost 10 years after the meeting.
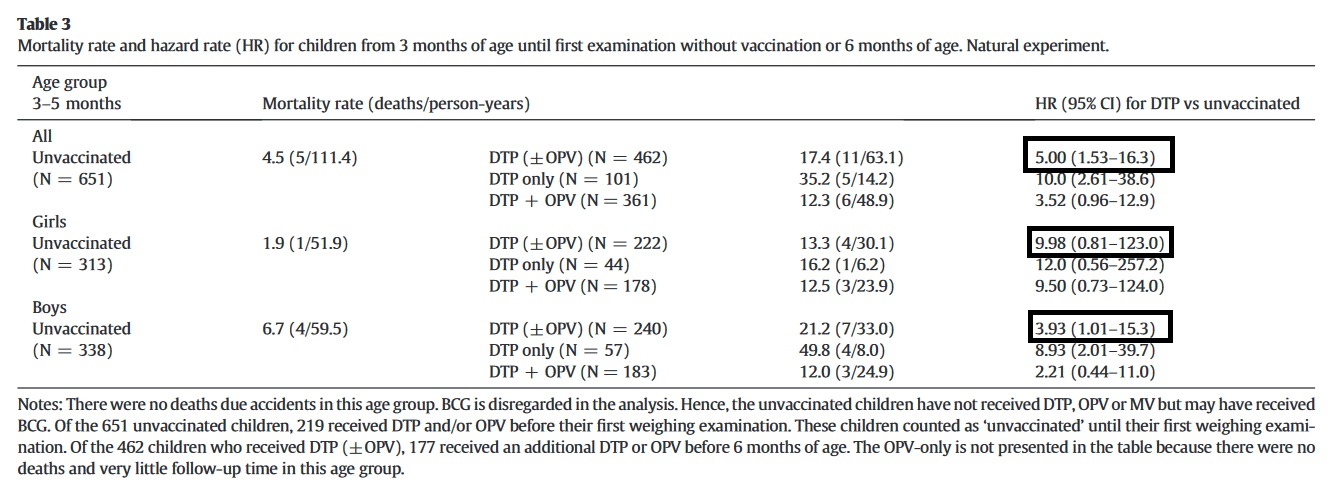
After the WHO revision, we went back to the old data. BHP had introduced DTP vaccine into the community in the 1980s, believing it would be beneficial. However, when we entered and analyzed the data, we found further confirmation of negative NSEs from DTP vaccine. The best data were for children 3-5 months old, because in this age group, as DTP vaccine was given at 3-monthly weighings, it was completely random (depending on date of birth) whether a child was vaccinated or not.
In dit "natural experiment" met gegevens uit 1981-83 hadden kinderen die DTP-vaccin hadden gekregen een 5 keer hogere sterfte dan kinderen die nog geen DTP-vaccin hadden gekregen. Dit was meer uitgesproken voor vrouwen (10 keer hoger) dan voor mannen, maar het resultaat was niet significant. Dit is waarschijnlijk het onderzoek waar Robert F Kennedy Jr naar verwijst.
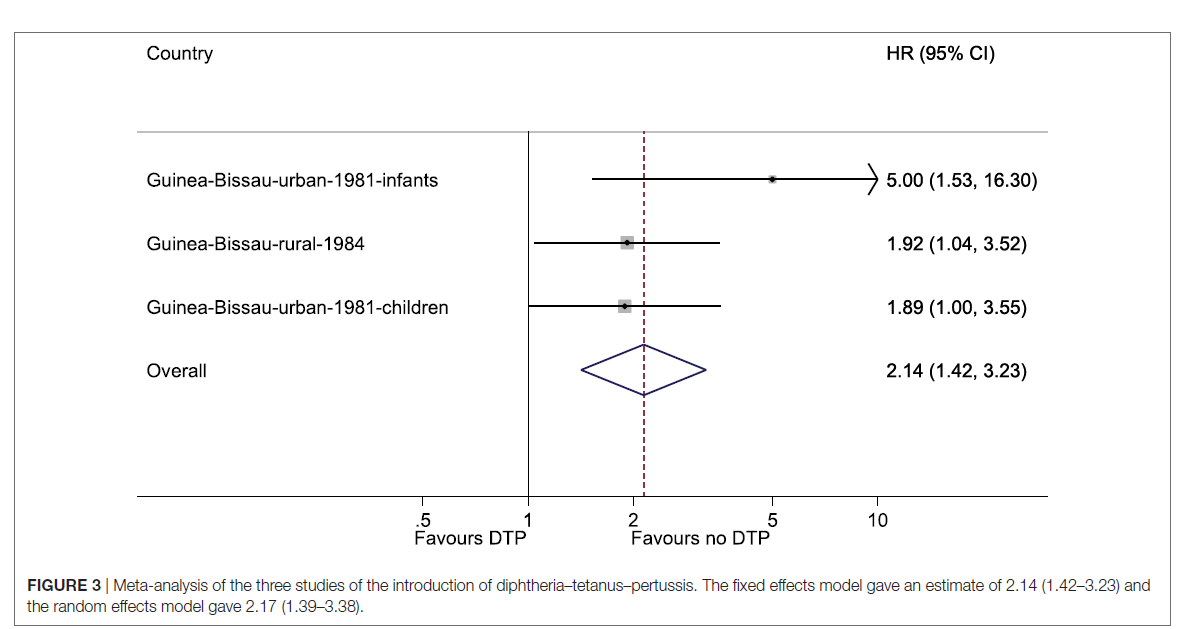
In later studies in older children over the same period, we found similar results, and in 2018 we published a combined analysis of the three studies which were carried out during the introduction.
The analysis showed that the introduction of DTP vaccine in Guinea-Bissau was associated with a 2-fold increase in overall mortality. In girls, the estimate was a 2.60 (95% CI=1.57-4.32)-fold increase in mortality. Remarkably, these studies were published after the WHO evaluation. If they had been included in the WHO evaluation, the negative effect of DTP vaccine would have been stronger.
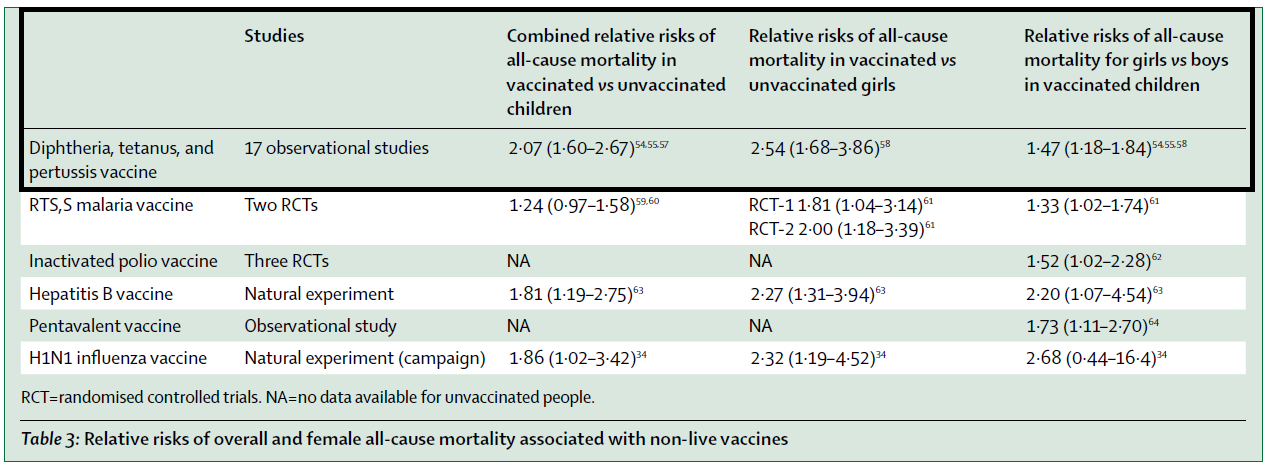
In 2020, we reviewed all data related to a Major review of non-specific impacts. Including all studies with prospective follow-up, including the new studies, for a total of 17 studies, being DTP-vaccinated versus not being DTP-vaccinated was associated with 2.07 (95% CI=1.60-2.67)-fold higher mortality. The estimate was 2.54 (1.68-3.86) in women. Among DTP-vaccinated children, women had nearly 50% higher mortality than men (1.47 (1.18-1.84)). There is a dose-response relationship observed, with the mortality rate in women and men increasing with each additional dose of DTP vaccine.
DTP is not the only vaccine associated with increased overall mortality among women. The same pattern has been observed for now six non-live vaccines (see table below). Importantly, the opposite pattern is seen for live vaccines. They are associated with favorable NSEs and lower overall mortality, especially in women. No bias can explain why only non-live vaccines would be negative for women.
Belangrijk is dat, aangezien de gegevens aantonen dat het negatieve effect wordt opgeheven wanneer een levend vaccin wordt gegeven, het mogelijk moet zijn om vaccinatieprogramma's te ontwerpen die de belangrijke niet-levende vaccins bevatten die beschermen tegen dodelijke ziekten, maar er gewoon voor zorgen dat kinderen zoveel mogelijk tijd doorbrengen met een "levend vaccin-laatst" schema.
In conclusion, Robert F Kennedy Jr is wrong that we were sent by the Danish government to study the effect of the DTP vaccine. Bill Gates was not involved. We are independent researchers, driven by an initial discovery that measles vaccine had highly beneficial NSEs.
Een van onze DTP-onderzoeken was een recente analyse van het "natuurlijke experiment" dat plaatsvond toen DTP-vaccin 30 jaar geleden in Guinee-Bissau werd geïntroduceerd. Hieruit bleek dat het krijgen van DTP-vaccin versus het nog niet krijgen van DTP-vaccin gepaard ging met een 5-voudig significant hoger sterftecijfer. Het was 10-voudig hoger voor vrouwen, maar het was niet onafhankelijk significant voor meisjes.
However, this is just one of many studies on DTP vaccine that all point in this direction. Most come from Guinea-Bissau, but the findings are the same in, for example, Benin, India and Malawi.
The conclusion is very clear: the whole-cell DTP vaccine used in low-income countries is associated with increased mortality among women. This observation is not contradicted by good prospective studies. What remains unclear is why the WHO is not taking action. That's why we're glad Robert F Kennedy Jr. is sharing the story about the DTP vaccine, even though he got some details wrong.
The following is a list of some studies showing negative nonspecific effects of DTP vaccine in women. No good research on DTP given without BCG and with prospective follow-up has contradicted the findings.
Want to know more?
TEDx over NSE's
A good article for laypeople that tells the story about NSEs
References
- Kristensen I, et al. Routine vaccinations and child survival: follow up study in Guinea-Bissau, West Africa. BMJ 2000;321:1435–8.
- Aaby P, et al. Routine vaccinations and child survival in war situation with high mortality: effect of gender. Vaccine 2002;21:15–20.
- Aaby P, et al. Differences in female-male mortality after high-titre measles vaccine and association with subsequent vaccination with diphtheria-tetanus-pertussis and inactivated poliovirus: re-analysis of West African studies. Lancet 2003;361:2183–8.
- Aaby P, et al. The introduction of diphtheria-tetanus-pertussis vaccine and child mortality in rural Guinea-Bissau: an observational study. Int J Epidemiol 2004; 33: 374–80.
- Aaby P, et al. Divergent female-male mortality ratios associated with different routine vaccinations among female-male twin pairs. Int J Epidemiol 2004; 33:367–73.
- Veirum JE, et al. Routine vaccinations associated with divergent effects on female and male mortality at the paediatric ward in Bissau, Guinea-Bissau. Vaccine 2005; 23: 1197-204.
- Aaby P, et al. Sex differential effects of routine immunizations and childhood survival in rural Malawi. Pediatr Inf Dis J 2006;25:721–7.
- Aaby P, et al. Age-specific changes in the female-male mortality ratio related to the pattern of vaccinations: an observational study from rural Gambia. Vaccine 2006; 24:4701–.
- Aaby P, et al. Increased female-male mortality ratio associated with inactivated polio and diphtheria-tetanus-pertussis vaccines: Observations from vaccination trials in Guinea-Bissau. Pediatric Infectious Disease Journal 2007; 26: 247-52.
- Aaby P, et al. DTP with or after measles vaccination is associated with increased in-hospital mortality in Guinea-Bissau. Vaccine 2007; 25: 1265-9.
- Benn CS, et al. Why worry: vitamin A with DTP vaccine? Vaccine 2007; 25:777–9.
- Benn CS, et al. Does vitamin A supplementation interact with routine vaccinations? An analysis of the Ghana vitamin A supplementation trial. Am J Clin Nutr 2009; 90:629–39.
- Aaby P, et al. Early diphtheria-tetanus-pertussis vaccination associated with higher female mortality and no difference in male mortality in a cohort of low birthweight children: an observational study within a randomised trial. Arch Dis Child 2012:97:685–91.
- Benn CS, et al. Diphtheria-tetanus-pertussis vaccination administered after measles vaccine: Increased female mortality? Pediatric Infectious Disease Journal 2012; 31: 1095-7.
- Aaby P, et al. Testing the hypothesis that diphtheria-tetanus-pertussis vaccine has negative non-specific and sex-differential effects on child survival in high-mortality countries. BMJ Open 2012; 2:e000707.
- Hirve S, et al.. Non-specific and sex-differential effects of vaccinations on child survival in rural western India. Vaccine 2012;30:7300–8.
- Krishnan A, et al.. Non-specific sex-differential effect of DTP vaccination may partially explain the excess girl child mortality in Ballabgarh, India. Trop Med Int Health 2013; 18:1329–37.
- Aaby P, et al. Sex-differential and non-targeted effects of routine vaccinations in a rural area with low vaccination coverage: Observational study from Senegal. Trans Roy Soc Trop Med Hyg 2015; 109:77–85.
- Higgins JPT, et al. Association of BCG, DTP, and measles containing vaccines with childhood mortality: systematic review. BMJ 2016; 355:i5170.
- Aaby P, et al. The WHO review of the possible nonspecific effects of diphtheria-tetanus-pertussis vaccine. Pediatr Infect Dis J 2016; 35: 1247–57.
- Aaby P, et al. Is diphtheria-tetanus- pertussis (DTP) associated with increased female mortality? A meta-analysis testing the hypotheses of sex-differential non-specific effects of DTP vaccine. Trans R Soc Trop Med Hyg 2016; 110: 570–81.
- Aaby P, Ravn H, Benn CS, et al. Child mortality after inactivated vaccines versus standard measles vaccine at nine months of age: a combined analysis of five cross-over randomised trials. Pediatr Infect Dis J 2016; 35:1232–41.
- Andersen A, et al. Sex-differential effects of diphtheria-tetanus-pertussis vaccine for the outcome of paediatric admissions? A hospital based observational study from Guinea-Bissau. Vaccine 2017; 35:7018–25.
- Welaga P, et al. Fewer out-of-sequence vaccinations and reduction of child mortality in Northern Ghana. Vaccine 2017; 35:2496–503.
- Mogensen SW, et al. The introduction of diphtheria-tetanus-pertussis and oral polio vaccine among young infants in an urban African community: a natural experiment. EBioMedicine 2017; 17: 192–98.
- Aaby P, et al. Evidence of increase in mortality after the introduction of diphtheria-tetanus-pertussis vaccine to children aged 6–35 months in Guinea-Bissau: a time for reflection? Front Public Health 2018; 6: 79.
- Hanifi SMA, et al. Diphtheria-tetanus-pertussis (DTP) vaccine is associated with increased female-male mortality rate ratios. A meta-analysis of studies of DTP administered before and after measles vaccine. J Infect Dis. 2020 Oct 30.
- Clipet-Jensen C, et al. Out-of-Sequence Vaccinations With Measles Vaccine and Diphtheria-Tetanus-Pertussis Vaccine: A Reanalysis of Demographic Surveillance Data From Rural Bangladesh. Clin Infect Dis. 2021 Apr 26; 72(8):1429-1436.
- Øland CB, et al. Reduced Mortality After Oral Polio Vaccination and Increased Mortality After Diphtheria-tetanus-pertussis Vaccination in Children in a Low-income Setting. Clin Ther. 2021 Jan; 43(1):172-184.e7.


"whole-cell diphtheria-tetanus-pertussis (DTP) vaccine [Note: the P stands for Pertussis = Whooping Cough, Not Polio]"
and further down it says this:
"Reception of DTP (almost always with oral polio vaccine) was associated with possible increases in all-cause mortality on average (relative risk 1.38, 0.92 to 2.08) from 10 studies with a high risk of bias; this effect seemed to be stronger in girls than in boys".
What is it now? The P of Whooping Cough or the P of Polio?
DTP jab (P = whooping cough) and simultaneously administered oral Polio vaccine. I will make that a little clear in the text.