
Vaxophile Netherlands is rebounding: yet another study that shows how beneficial the vaccines were. This time I will stick to discussing statements from the press release and the study itself. These did not give reason to delve further into the figures. That takes me a lot of time and others can do it better than I can. It doesn't matter, Keulemans just keeps shouting anyway and the legacy media is still the Single Source of Truth for the vaccinated. But ZonMW finances that propaganda content from our tax money. Can't they at least use a quality threshold?
The press release
Some phrases from The accompanying press release UMC:
"The results show that someone who was vaccinated was on average 44 percent less likely to die in the three weeks after vaccination than in the weeks after."
- This means that a vaccination that is only considered effective after two to three weeks is less effective after those three weeks in terms of 'risk of death' than in the first three weeks that are ineffective. This may be called a striking finding, especially since a vaccination should not have any systemic effect immediately after the jab (apart from the bizarre numbers). The obvious explanation is the HVE (Healthy Vaccinee Effect). People who were expected to die within one or a few weeks were no longer vaccinated. Then as a jabbed person you are left with only those who have a lower mortality rate, especially where the first few weeks are concerned. This is not due to the vaccination but to the selection of whether or not to vaccinate. This statement is underlined again in the report itself, I will come back to that.
- How do you recognize a Healthy Vaccinee Effect? If a large difference occurs immediately after a medical intervention for no apparent reason that fades away over time. That is accurately described here.
“Higher mortality risk after infection
The study also shows that the risk of death in the first three weeks after a corona infection was 16 times higher than in the weeks that followed."
- A sideline because here they rub the seriousness of a corona infection under our noses, as if it is still responsible for excess mortality. At least that's how it seems. But something similar applies to numerous causes of death, take the fall from a kitchen ladder. More people die from it in the first three weeks after the fall than afterwards. The relevance of that observation is therefore not entirely clear to me. Scaremongering, in the form of "it was really very serious"!? That could be, but we already knew that people have died of Covid. That this usually does not happen after a few months. A meaningless fact in this study.
"The temporary activation [of the immune system] can, in rare cases, be associated with serious side effects, including myocarditis, thrombosis and neurological complications."
- It is not the temporary activation of the immune system that causes side effects. Side effects are associated with it, but that is due to the uncontrolled distribution of varying amounts of spikes throughout the body and possibly the DNA pollution, although this is a long-term issue. The fact that an investigation into these side effects is limited to the first three weeks is questionable to say the least. Also because we are still seeing substantial excess mortality while, apart from the autumn shot (about 22% of the population), there has not been a vaccination for a long time.
The research report
https://www.medrxiv.org/content/10.1101/2024.12.11.24318790v1
"The authors have declared no competing interest."
- We see among the authors various hardcore corona vaccination pushers, members of vaccination alliances, think tank disinformation – in short, sources that have propagated a lot of misinformation. That there are no competing interests is therefore not correct. Just think of the possible reputational damage for the vaccine promoters.
"Whether COVID-19 vaccination contributed to excess mortality has been investigated in several countries, consistently showing no increased risk for non-COVID-19-related mortality and a protective effect for COVID-19-related mortality."
"This design focuses on the immediate period after vaccination, in which immune activation can increase the risk of serious side effects, resulting in death. Despite this, those [foreign] studies consistently show a lower risk of death from any cause after vaccination compared to non-vaccination periods."
- Other studies that show no risk often measure HVE. People who see their end of life approaching are no longer vaccinated and die unvaccinated, also from causes other than Covid. The fact that the healthier vaccinated people die less is then attributed to the effect of the vaccination. In addition, there are also studies that do show negative effects (including mortality). The authors are apparently not aware of those studies. In the Netherlands, we also have the data pollution due to misregistration of deceased people shortly after vaccination (see The chaos of the numbers and more on the site of Herman Steigstra).
- More about that HVE in the previous articles "Kaplan-Meier voor Dummies“, “A statistical fallacy in Italy and at Nivel" and "HvE for dummies".
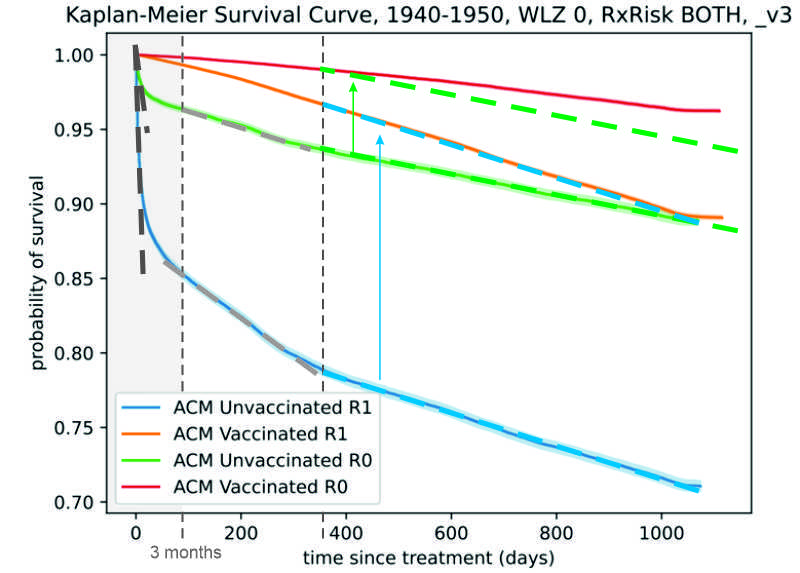
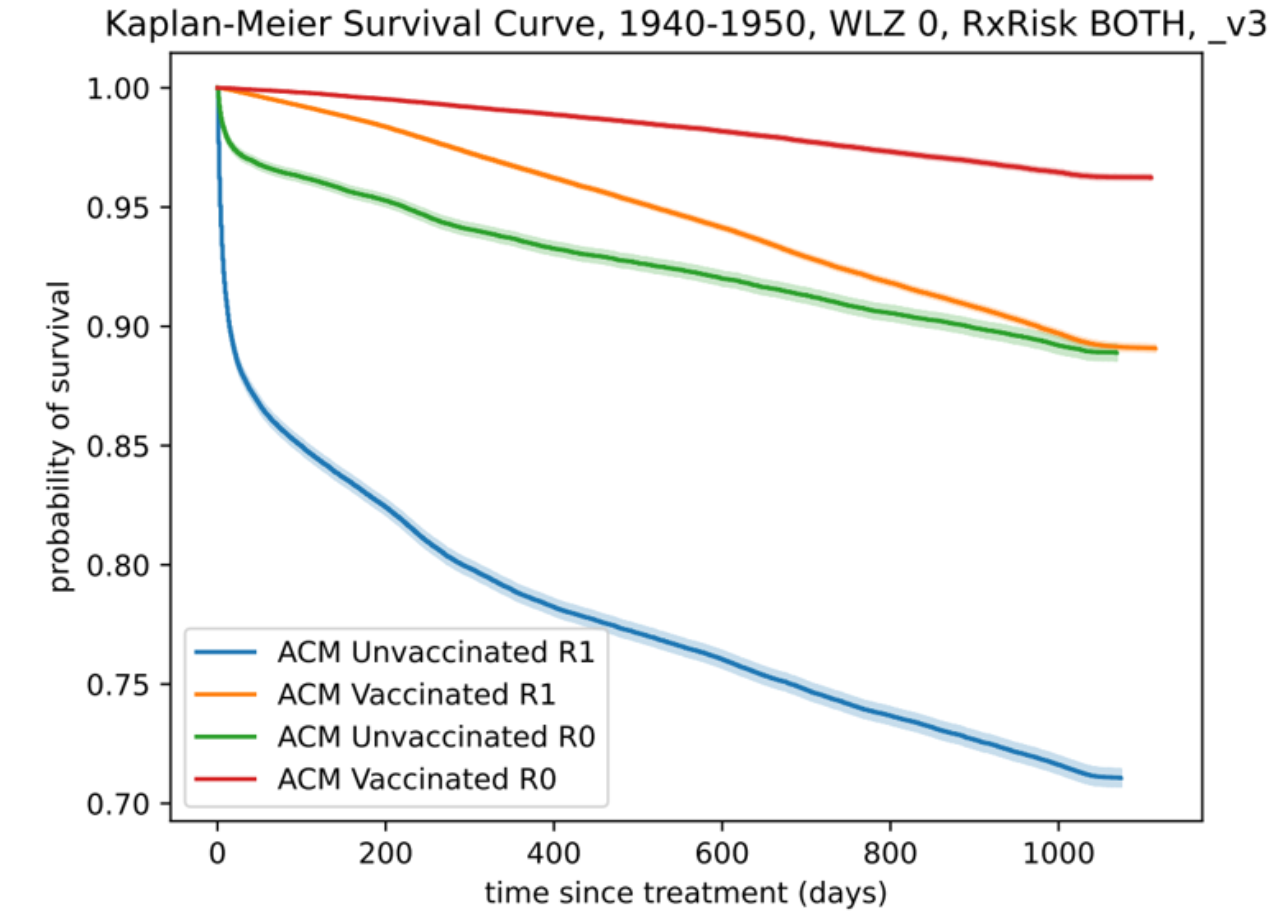
- Below you can see what can be seen in CIMS in the first weeks. Huge mortality among unvaccinated people in the first week. These are largely people who have been taken OUT of the vaccinated group due to registration problems and the HVE. No wonder that vaccinated group performs better. As the "unvaccinated" line flattens out, the effect decreases. After just a few months, it doesn't really make that much difference. That difference could even be HVE. Which could mean for the orange line that the healthy unvaccinated die less than the equally healthy vaccinated.
"For the analysis of the effect of a positively registered SARS-CoV-2 infection, residents were selected who died between June 1, 2020 and December 31, 2021, in the period in which the tests were registered."
"At the time of the study period, COVID-19 was a notifiable disease in the Netherlands, which means that all positive SARS-CoV-2 infections had to be reported to a municipal health service."
- Measurements were taken on the basis of registered infections. Here it is suggested that every infection was registered because it was mandatory. Of course, that did not happen that way: many did not or hardly noticed that they were infected. These millions of people who have had an infection without it being registered were not included in the study. They have not been to a doctor or a hospital. Everyone who did end up in hospital, on the other hand, was tested for corona and with the high prevalence of the virus, this automatically leads to many registrations among people who are not in good shape, for whatever reason.
"COVID-19 vaccination data were obtained from the COVID Vaccination Information and Monitoring System (CIMS) (2020-2023)".
- Much has already been written about the polluted data in the CIMS, and the Nivel study also came to the wrong conclusions. Discussions on this issue are still ongoing.
"The baseline series was considered complete and effective 14 days after a subject received two or three (indicated only for immunocompromised individuals) primary vaccinations."
- So despite the vaccinations being considered effective only after 14 days, they showed a substantial reduction in mortality in the first week. (How can you write this!?)
"With death as an event of special importance, the key assumptions of a standard SCCS are violated, as death excludes subsequent exposures and observation periods. This modified SCCS compares the risk of death during a predefined risk period after exposure with a reference period, defined as all the observation time during which subsequent exposures could have occurred. This makes the end of the observation period independent of events. The model is estimated by iteratively reweighting observations to align them with a counterfactual scenario in which no exposures can occur after death, ensuring that death does not censor exposures, as there are no exposures in this counterfactual scenario."
- I have read this 5 times but I would like to have this explained to me by someone who understands it better.
"Analyses for the baseline series were additionally stratified for vaccine type (mRNA or nonmRNA/unknown), and a previous registered positive SARS-CoV-2 infection before vaccination (yes/no)."
- Apparently, everyone who has had the bassiserie has been recorded whether or not they had had a previous infection. I did not know that the basic vaccination was accompanied by a serological test for antibodies. (Why you were vaccinated at all despite a previous infection, we still don't know, by the way.)
This one is really very special:
"The relative incidence ranged within the risk interval from 0.33 (95%CI 0.31-0.34) at week one, to 0.56 (95%CI 0.54-0.58) at week two, to 0.73 (95%CI 0.70-0.75) at week three."
- So:
Week 1 after the shot: 33% of the normal chance of dying
Week 2 after the shot: 56% of the normal chance of dying
Week 3 after the shot: 73% of the normal chance of dying
So here it is claimed with dry eyes that you were 2.5 times more likely to die three weeks after the shot than in the first week after the shot.
That sounds familiar to us and it confirms that we are dealing with the HVE here. The people who had at most a week to live have not been vaccinated. Of people who were in a less bad state, a little more will have been vaccinated. In short: the longer the horizon, the more often one was pricked. This explains why mortality among the vaccinated was lowest in the first week and why it rises again over time. The imminent deaths have simply been filtered out. It has absolutely nothing to do with the effect of the vaccinations.
"The differences between individuals who died within three weeks of vaccination and those who died in the period thereafter were small."
- This indicates that a probable date of death is more difficult to determine the further into the future that date is. 1 week is easy to determine, two weeks too but after that it becomes difficult.
"The relative incidence was slightly stronger for individuals vaccinated by municipal health services (IRR 0.46, 95%CI 0.44-0.48) or general practitioners (IRR 0.55, 95%CI 0.52-0.59), compared to individuals vaccinated by other administrators (IRR 0.77, 95%CI 0.74-0.80)."
Here the impression is created that those who stung had an influence on the effect of the shot. That is undoubtedly the same line of thought, because at the GGD the average population has been vaccinated, at the GP people with complaints, in the hospital people with even more complaints. The vaccination selection is again reflected in the mortality rates.
Disclaimer
The data pollution is a bridge too far for these researchers. But did they also have no idea of the Healthy Vaccinee Effect at all? Yes, it is:
"This HVE (effect of healthy vaccinated people) may slightly overestimate the reduction in deaths after vaccination and point estimates should therefore be interpreted with some caution."
But they have made no attempt to correct for this. Nor is that possible, because there is a risk that all observed effects will be corrected away.
A lot of dust is being raised, it seems. It is becoming more and more cramped. If it's not the, what is it? It seems like a rearguard fight to me when you see what is happening in America at the moment.
Saw this one at Campbell: https://doctoraseem.com/thousands-of-doctors-sign-petition-to-suspend-covid-mrna-vaccines-an-open-letter-to-the-gmc/
A number of anonymous doctors have sued Malhotra at the GMC (General Medical Council), but they did not take action. They then sued the GMC. This letter is very strong.
You will have read it too. What they produce in terms of 'vaccine' propaganda here in our cool country is becoming less and less relevant, I think.
I think a side effect is not yet known. Corona vaccines will make you lie and make you unscrupulous.
These people don't seem to have any problems at all that they are engaged in a genocide. They participate in the medical world that was created for the protection of people. Apparently nothing is sacred anymore these days.
Nice piece Anton. Just a little farmer's sense against it, and the sandcastles collapse!
Scss stands for self-controlled case series. In this observational research design, individuals are compared with themselves. This corrects so-called fixed confounding variables such as genes, gender, socio-economic status, (to a certain extent) age and other variables that someone always has (e.g. medication, chronic disease) in the model.
To put it more simply: with cohort studies you compare human 1 with human 2 (apples vs oranges). With Sccs you compare human 1 with human 1 (apples vs apples). The only thing that varies in scss is the time.
What authors have done with this scss is looked at a group of people who have died (outcome) at 2 time periods when they died. Time period 1=just after vaccination (up to 3 weeks after vaccination). Time period 2=a while after vaccination (>3 weeks after vaccination). It then appears that more of the deceased people died in time period 2 than in time period 1 (corrected for length of time = duration with a so-called incidence rate)
From the abstract: 'We found a 44% lower relative incidence of all-cause deaths in the first three weeks after the primary vaccination compared to more than three weeks after vaccination (IRR 0.56, 95%CI 0.54-0.57).'
Most common explanation for the relative risk found:
1. Someone is only vaccinated if they still have something of a life expectancy (more than 3 weeks). Even in an elderly/nursing home, the average life expectancy is half a year (where vaccination was done), in the ICU or in terminal cancer/hospice it will be less than 3 weeks and those people were (I assume) not vaccinated (that often). In other words: this finding (of less mortality just after vaccination) was also found for placebo.
Missed opportunity: what was the IRR in unvaccinated people? – So if, for example, you had put a control person at time x of person 1 who receives the vaccine who had not taken a vaccine (and matched on factors such as age, gender, ... HVE) and had followed over the same 2 time periods. – Then you might have found an even lower IRR than 0.56 (because most people have a life expectancy of >3 weeks). Then you could have divided IRR vaccinated (=0.56) on IRR unvaccinated (IRR= we don't know, but probably lower than 0.56 which could have given the relative risk of mortality on vaccinated vs unvaccinated in the first 3 weeks after vaccination.
Other reasons I think of off the cuff for the result I found
2. The vaccinated people who died immediately after the jab are not/are undertested in the dataset
3. Data torture. The model that is used is not really straightforward, I wouldn't be surprised if a statistician pressed/had to press a button until the 'correct' answer came, after which the other authors quickly proceeded to write the roaring conclusions
Thanks again, reading a good piece about the fiddling with data (to put it bluntly) takes the edge off my primary reaction. How long will this huge scandal last? And unfortunately, more and more rubbish is being added. Fortunately, no mrna stuff for humans (yet), but now administering antibodies to all babies from 2025 is also called vaccines. Creeps like Patricia brownish (also became a professor in Utrecht) are responsible for this. Still, I think that a lot of people now hear a tiny voice that says that it is all wrong. Partly thanks to sites like this one.
Yesterday I already congratulated the UMC editors for showing that after three weeks the mortality due to vaccination increases enormously and that the low mortality in the first three weeks is partly caused by the H'V'E (large).
I'll be very honest. I don't understand it anymore with so much information. I'm also not good at statistics etc. In fact, I'm just not at home in it. However, I know which people are right to make their point and who are not. And those are the people who want to serve humanity again and again and investigate everything with integrity and with the right objective. Thank you for that. Many thanks For me it is a matter of life experience and which people I have met in my life, so I also know who is lying and who is not. Here they are not lying and a few more sites. I dare to put my hand in the fire for that.
This is what chatgpt says about the text to be explained:
This text refers to a statistical model, the so-called "SCCS" (Self-Controlled Case Series), which is used to study the effects of exposures (e.g. medication or vaccination) on health outcomes (e.g. illness or death). In the context of the text, this model is modified because of the effect of death, which can interfere with normal observations in a standard SCCS.
**Simplified explanation:**
1. **Death as a special case:** The standard SCCS model looks at events such as illness or death in a certain period of time after exposure to a risk factor (e.g. a vaccine). Normally, the model would then compare the events with periods in which there was no exposure. However, when someone dies, it can interfere with the analysis because that person cannot undergo further exposures or observations after death. This is the problem the text refers to: death excludes future exposures and observations.
2. **Custom SCCS model:** The model is thus modified to take into account death as a special case. Instead of only looking at the period immediately after exposure, this modified model compares the risk of death in a predefined risk period (e.g. within a few months after exposure) with a reference period. This reference period is the time during which other possible exposures could have occurred.
3. **What does "independent of events" mean?** The model thus makes the length of the observation period independent of events such as death. This means that the observation period does not end when someone dies, but continues until the end of the risk period (for example, the predetermined months after exposure).
4. Iterative reweighting: The model is then analyzed by "iterative reweighting," which means that the observations (data) are repeatedly adjusted until they match a scenario where death does not affect exposures. This is called a counterfactual scenario – a hypothetical scenario in which death has no effect on the potential for future exposures.
5. **Why is this important?** The purpose of this adjustment is to ensure that a person's death (which would normally lead to the cessation of observation) does not affect the results of the analysis, because in the counterfactual scenario (where death does not play a role) no further exposures can occur after death.
In short, this text explains how the SCCS model is modified to account for death, so that the model can provide reliable results without deaths interfering with observations.
Do you understand what ChatGPT writes? I can't imagine it very well.
ChatGPT also says: "The SCCS method has an important limitation in irreversible outcomes such as death after an intervention, because you cannot have a direct control period in which mortality is measured before the intervention (after all, these people cannot have undergone the intervention). As a result, SCCS is less powerful or even not applicable in this specific case, unless you make adjustments, such as analyzing different periods after the intervention. In practice, cohort studies or survival analyses are often better suited to conduct this type of research."
When researching the autism-vaccination relationship, I get it: you compare the incidence in the three weeks before the shot with the three weeks after the shot. That is not possible with death. If the incidence is before the injection, you will never be in the research group again. Or you have to come up with fictitious pricking moments: slippery ice. If you compare with the period after 3 weeks, you have already lost everyone who died within 3 weeks, so that also skews things (survival bias). Complex.
And there is no danger in "iterative reweighting": making adjustments until... etc.?
Anyway, fodder for methodologists. We don't even have to dig that deep here.
Anton
Thanks for your comment.
I have also read ChatGPT's response a number of times.
I took out that the authors of the report have applied a "self-invented" new way of calculating.
For me, it means in a nutshell:
"The current ways of calculating do not give the outcome we need, so come up with a ruse."
It's a bit short-sighted, but you do get that impression. All statistical boxes of tricks must be opened.
I have put the UMC research through its paces together with ChatGPT. The conclusions are even worse than have already been mentioned by Maurice, Anton and Herman.
In these SCCS, the sensitivity analysis of the induction period also indicates a high degree of randomness of mortality around the time of vaccination. And therefore no relationship with vaccination. And that is not mentioned in the study.
Furthermore, the previously published criticism of this study (the vaccine as an "elixir of life", errors as a result of the Healthy Vaccinee Effect and under-registration of vaccinated people) has been further substantiated and illustrated with numerical examples.
Below is a summary of the findings. AND in the link the complete conversation with ChatGPT.
Main findings of the
Excess mortality – Vaccination study of UMC
Link to this document: Key findings of the Excess Mortality Vaccination study of UMC.docx
https://janvdzanden-my.sharepoint.com/:w:/g/personal/jan_janvdzanden_onmicrosoft_com/ETbow4iYVVFGrfDzw8KrbHkBwfcHMLQA25YZSgLpiX2E-A?e=u4OKAB
The all-cause mortality in a "self-controlled case series" of all deaths from June 2020 to December 2023 was examined. I.e. only the population of vaccinated people has been looked at. As a result, bias and distortion are (more or less) excluded, according to the authors; errors in the registration of vaccination should then have no influence.
I (with ChatGPT) think differently, because there can be several errors in selection, healthy vaccinee effect and methodology, so you would have to do a major correction and/or a similar study in unvaccinated people to be able to draw reliable conclusions.
The attachment contains an extensive conversation with ChatGPT.
The conclusion is that based on all the studies currently known, the hypothesis that excess mortality is caused by side effects of the vaccine is more plausible than that it is due to other effects. Both Nivel and UMC research are being questioned by ChatGPT because of intrinsic contradictions of data and conclusions.
The UMC research raises some fundamental questions.
How can 44% (67, 44, 27% in weeks 1, 2 and 3 respectively) die in the 3 weeks after vaccination than in the long period afterwards? (p. 6, 2nd paragraph) Even if there is no Corona (because the sensitivity analysis shows that conclusions apply over the entire time series)? Then the vaccine is a kind of "magic potion", which ensures that you die less from all causes for 3 weeks. That can't be, can it? Question 1: ChatGPT explains this by a combination of HVE and registration errors of vaccinated and unvaccinated people
And how can 51% fewer people die in the 3 weeks after the booster than in the long period afterwards? (p. 6, 3rd paragraph). Same incongruity as the previous paragraph. Question 1.A.
And further: isn't it strange that a vaccine that is intended, among other things, to reduce mortality from Corona and, according to studies, only works after 2 to 3 weeks, is (very) effective for the first 3 weeks, even against dying from diseases for which it is not intended at all, and then apparently no more? Question 1.B ChatGPT cannot explain this either.
Logically, the increased mortality rate within 3 weeks after registered infection seems to be 16.2 times as high (...? ...., 22.6, 9.9 in week 1, 2 resp. 3) than in the long period after that (5th paragraph). This is broken down: for vaccinated people in the 6 months prior to it, the mortality rate is 6.1% and for unvaccinated people 16.9%. Because there are many more (about 85% vaccinated) than unvaccinated (about 15%), that can't be an average of 16.2% (previous paragraph)? How is this possible? Question 2. ChatGPT cannot explain this either, but suspects that something has been done with weighting factors; But that is not mentioned and therefore not transparent.
It seems logical that mortality is higher among the elderly (20.6%) than among young people (2.7%). Given the proportions, that could also come to an average of 16.2%. The slightly higher risk of men than of women, and the increase in (co)morbidity is also logical and also comes to an average of about 16.2%.
What does it say here: "Furthermore, setting the induction interval to 2, 4, 7 or 14 days before the registration date attenuated the relative incidence (IRR 14.79, 13.02, 9.91 and 2.54, respectively). " Here it says (see explanation by ChatGPT) that sensitivity analysis shows that most mortality around the time of vaccination has nothing to do with the vaccination itself but with other causes. So this almost completely undermines the power of the findings. Why is nothing said about this in the report? Question 3. According to ChatGPT, this should absolutely be mentioned in a good study and, if possible, explained, because it greatly undermines the robustness of conclusions.
Page 8 (Discussion, last paragraph)) mentions that the 7 resp. 5% registration errors have no influence because unvaccinated people fall outside the scope of the study. But on p. 6 et seq. it is repeatedly stated that unvaccinated people have a higher mortality risk than vaccinated people.
That's not right, is it? Precisely because the vaccination rate is quite high (about 85%), an error of 7% on that 15% of unvaccinated people has a very big influence of up to 50%! And the Conlcusion also states that the study provides evidence that vaccination is not related to excess mortality; Of course with regard to the mortality of the unvaccinated. So there, too, the group of unvaccinated people is involved in the analysis/conclusion. Then a 50% error in the size of unvaccinated people is not negligible, is it? Question 4. ChatGPT states that in an SCCS, where there is no HVE and/or underregistration of sicker people, the registration errors of 5 and 7% respectively are indeed irrelevant. Unless those "privacy refusers" are not representative of the entire population.
Hello Jan,
Do you mind if I make a Post of this? Or maybe you want to go through the text yourself?
Make something beautiful out of it! I'll check afterwards if it's correct. Will you send a link?
Interesting isn't that analysis of ChatGPT.... 50 p. College Advances Statistics......
On LinkedIN I have it with better layout and layout.
You refer to a ChatGPT link, I can't find it. All links point to the same message.
The link refers to a .docx document that includes the complete chat.
Hi Anton,
I had Claude 3.0 (AI) do a thorough analysis on 3 NL reports and international reports on the effectiveness of vaccinations. The results are staggering. As I had understood from others before: vaccination has a negative effect among young people (50-). For the elderly, there may be a positive effect, but very much less than reported by the "official" reports. Read and shudder along.....
UMCU and NIVEL report analyzed by Claude 3.docx
https://janvdzanden-my.sharepoint.com/:w:/g/personal/jan_janvdzanden_onmicrosoft_com/Ed5cZVnL9eREvy5COMQIvZ8B_OypeZtPa_OxiN1EyyT5_Q?e=ogPrqf
Gosh this is very dramatic. Did you perhaps have him make a summary? This is quite difficult to read.
Not surprising this dramatic conclusion, which is largely based on what I think are one-sided figures.
Why is that not surprising? A vaccine against the flu may make sense for unhealthy people over 60 and, according to some, at most for people over 65 or 70. Covid 19 was about twice as severe as a (severe) flu in the beginning and less severe as early as 2021. If you look at hospital admissions in 2020, it appears that between the ages of 50 and 60, the number of admissions halved compared to people in their sixties. And in forty-somethings it halves again compared to fifty-somethings etc etc.
With a positive effect (tipping point) of 60 years with flu, that tipping point should theoretically be around 50 years with covid. But the virus was already less deadly at the beginning of 2021 and a minimum age of 55 or 60 years would have made more sense. Moreover, more than half of the population, especially the somewhat younger people, had already had covid one or more times in mid-2021. They were already much better protected at that time because the shots offered at most at least temporary protection against a virus that had not been present for a year and antibodies built up through infection are ten to twenty times more effective and remained and remain effective for longer.
That's right.
A correction: these are not one-sided figures. That's the treacherous thing. The figures themselves are not incorrect.
But because of the HVE effect you have to be careful about drawing conclusions directly from the figures. And AI {at least Claude] is now smart enough to be able to correct that properly. Apparently not those doctors and epidemiologists from UMCU, Nivel and CBS. Sad. Or is it on purpose……. But I still fear/think it is ignorance.
In addition, there is the pollution of 5/7% privacy refusers; but due to the design of UMCU, this does not play a role there.
And the errors in CIMS and the 2 or 3 week waiting time do not play a role in principle, because those effects are also corrected thanks to the HVE correction.
I'm curious what our real specialist thinks about this: Herman Steigstra.
But I think he had already performed similar calculations with correction much earlier...
.
In the beginning, the first 6 pages. Quite a fairly clear summary?
Maar je hebt gelijk: het is hard core statistiek. En dat is voor velen te lastig.
Ook voor de auteurs van het UMCU rapport!!