
Een vast onderdeel van elke wetenschappelijke publicatie is de sectie 'conflict of interest'. Ontvangt iemand bonussen of subsidies van partijen die belang hebben bij het werk, dan moet dat worden vermeld. De ICMJE (International Committee of Medical Journal Editors) ziet daarop toe. Dus is er een plotselinge grant of incidentele donatie, dan gaan er rode vlaggen omhoog en moet dat erbij staan. Zijn er andere banden met een belanghebbende partij (lezingen, consultancy) dan moet ook dat worden vermeld. Want persoonlijke financiële banden van hoofdonderzoekers met bijvoorbeeld een fabrikant leiden gemiddeld tot een ruim driemaal hogere kans op positieve uitkomst.
"Zeker", say the proponents then, "dat is toch fijn, meer positieve uitkomsten! Dat komt omdat je dan de echte experts erbij betrekt, die kunnen zo'n onderzoek laten slagen waar anderen de mist in gaan."
What does not have to be mentioned is total financial dependence. So if you get some occasional, bribery is lurking, but if you pay your mortgage, there is nothing wrong. The ICMje classifies a government or university salary, a business car and holiday pay not as a "financial conflict or interest". This dependence is therefore also due to the in combination with not seen as a reporting. Who would otherwise have to pay the trials? And all those committees and authorities that have to approve it all? The pharmacists also largely pay that, with the only reason that they have a financial interest in well -minded supervision. That is a mutual interest: the supervisors need the pharmacy cash flow to maintain itself and the pharmacy can flourish if the supervisors do not put salt on every snail. The supervisory authorities, very concrete: the income of supervisory officials, therefore depend on the infusion of the pharmaceuticals they must assess.
What that has led to you can be followed on the substack of A Midwesterndoc, this article for example.
In short: the system is not corrupted but financial dependencies structure the system. Why is that in those guidelines? That goes without saying: those guidelines have been drawn up by the same journal editors and research institutes that have hung their existence on that industry.
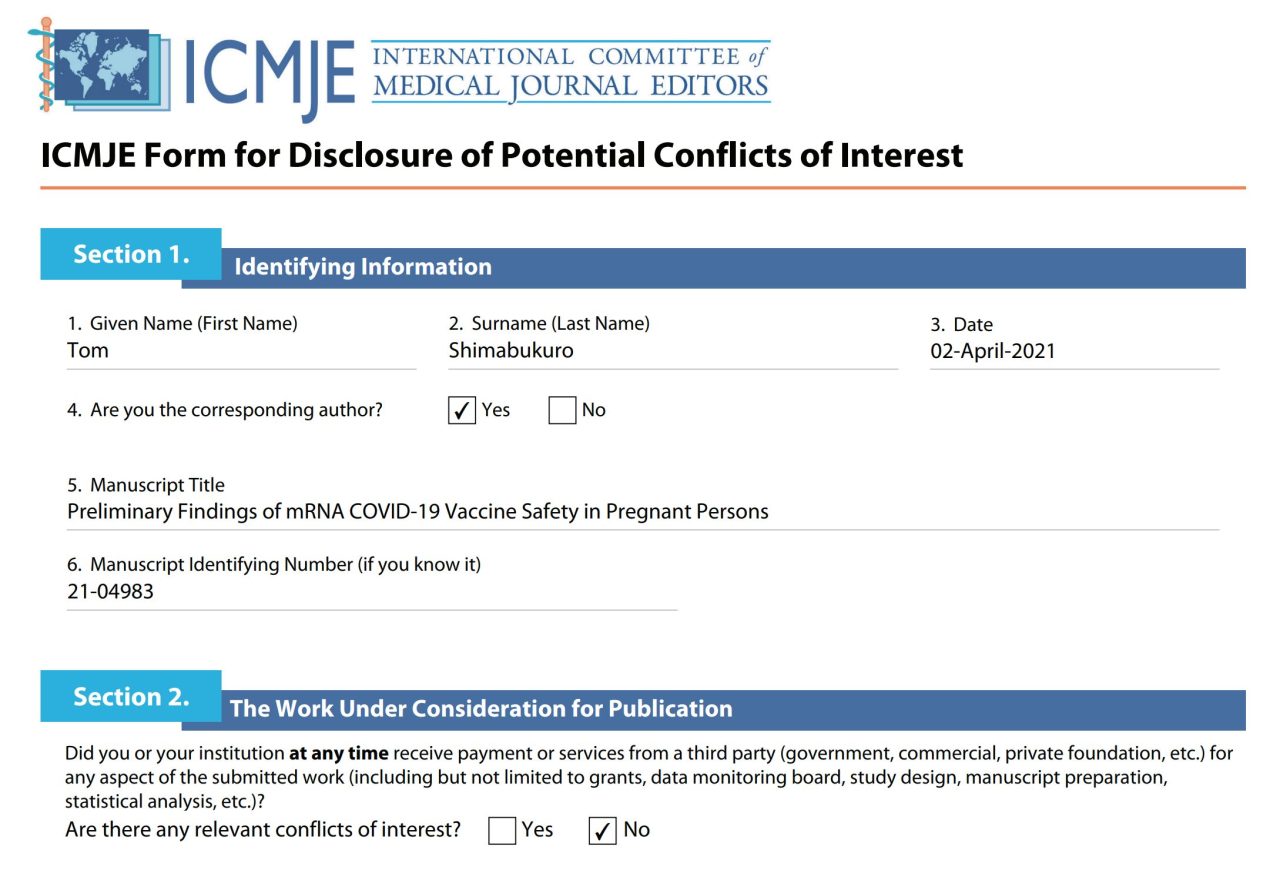
In a previous article1Viralvaria (Pregnancy and vaccinations: 45% more miscarriages in week 8-13 (IL), 30% more overall (CZ)) possible connections between vaccination and miscarriages were discussed. The first part was about the interpretation of a CDC study2Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons met enorme impact - nu nog steeds en destijds helemaal. De dubieuze onderzoeksopzet en de kritiek daarop3Virusvaria: https://virusvaria.nl/legacy-science-en-pro-vax-fraude-een-horrorvoorbeeld/ is al eerder aan bod gekomen. Ook besteedden we aandacht aan het recente advies van de Hoge Gezondheidsraad in België, om Pregnant women with a mrna/covidprik to be damaged.
Whether the vaccinations are safe for pregnant women is not so much under discussion here. The point is especially: early in 2021 the course was determined by an American study4The controversial study of Shimabukuro: https://www.nejm.org/doi/10.1056/NEJMoa2104983 They concluded that pregnant women had to be vaccinated. The CDC and FDA thus gave well -founded advice and did all authorities in the rest of the world (with us: EMA and the MEB) to take over this advice?
En vooral: waren de betrokken onderzoekers van de onderzoeken wel de aangewezen personen om zulk gevoelig onderzoek te doen? Een oefening in gezond verstand, geen gegoochel met noemers en tellers (voor degenen die niet zo sterk zijn in het onthouden van bijvoorbeeld wat de x- en wat de y-as is in een grafiek, of wat de teller en wat de noemer in een breuk.)
Chief researcher Tom Shimabukuro
Who were any stakeholders in this investigation? These were the pharmacists and the government endings and doctors who also recommended the Covid vaccinations to pregnant women.
Dr Shimabukuro, lead researcher of that crucial study, indicated that he had no conflicts of interest with the research.
Op dat moment hadden het CDC en de FDA zwangere vrouwen gewoon laten meelopen in de vaccinatiecampagne. En dat terwijl ze waren uitgesloten van de trials: er was niets bekend over zwangerschap en deze vaccins. Medisch personeel injecteerde zwangeren dus met experimenteel mRNA. ("experimenteel" zegt meer over de persoon die het krijgt dan over het goedje dat wordt ingespoten. Het argument dat mRNA niet meer experimenteel is omdat er al héél veel mee is geëxperimenteerd, is simpelweg niet valide.)
While pregnant women is always very careful, loving. On the patronizing. Below a list of what they are not allowed.
☒Filet americain, carpaccio, sushi with raw fish - risk of toxoplasmosis of listeria.
☒Raw milk cheeses: rather not because of listeria bacteria.
☒Be careful with liver (products): a lot of vitamin A, can be harmful to the baby.
☒Alcohol is out of the question: risk of Fetal alcohol syndrome.
☒Be careful with coffee, tea, energy drinks (too much caffeine), long -preserved fish and vegetables (Listeria).
☒Tuna, swordfish, shark, mackerel sometimes do not contain too much mercury during pregnancy.
☒Drop, a lot of salt: can increase blood pressure, which may have a negative effect on the development of the child.
☒Smoking (also moor smoking) is an absolute no-go (linked to cradle-death).
☒Medicine use (always consult with doctor/pharmacist, eg ibuprofen: not during pregnancy!).
☑Experimental genetically modified mrna vaccines (vaccines are safe)
☒Sauna, hot environments.
☒Avoid exercising with fall risk or heavy efforts.
☒Note with hair spray and cleaning products, these can contain harmful substances.
The green check mark is substantiated with the consensus that vaccines are safe and effective. Again: pregnant women were excluded from the trials. Nothing was known about pregnancies and C19 vaccinations. Certainly in view of the many menstrual problems and other Vaers reports (we speak at the beginning of 2021) it was therefore important that a peer reviewed positive investigation would appear on the effect of the MRNA vaccinations on pregnancy. That gap had to be filled quickly with good news.
Especially for the Deputy director of the H1N1 Vaccine Task Force at the CDC, who works as Coordinator for pandemic flu vaccination in the Immunization Services department of the CDC, that of life great importance.
Want to guess who that CDC CEO was three times?
Right: Dr. Tom Shimabukuro: the main investigator without conflict or interest.
It just indicates how the sector (and therefore science) works.
The V-Safe Data: so hopeful that it is worrying
The Shimabukuro study is based on data from V-Safe. Every vaccinate was given the opportunity in the US to download the V-Safe App in which the health status could be kept and side effects could be reported. A number of pregnant women also participated, say from January, February. In April 2021 the article was published that made vaccines safe with pregnant women.
In Table 4 of the study5The controversial study of Shimabukuro https://www.nejm.org/doi/10.1056/NEJMoa2104983 We see that dead births in the vaccinated V-Safe women were surprisingly less common than the national average.
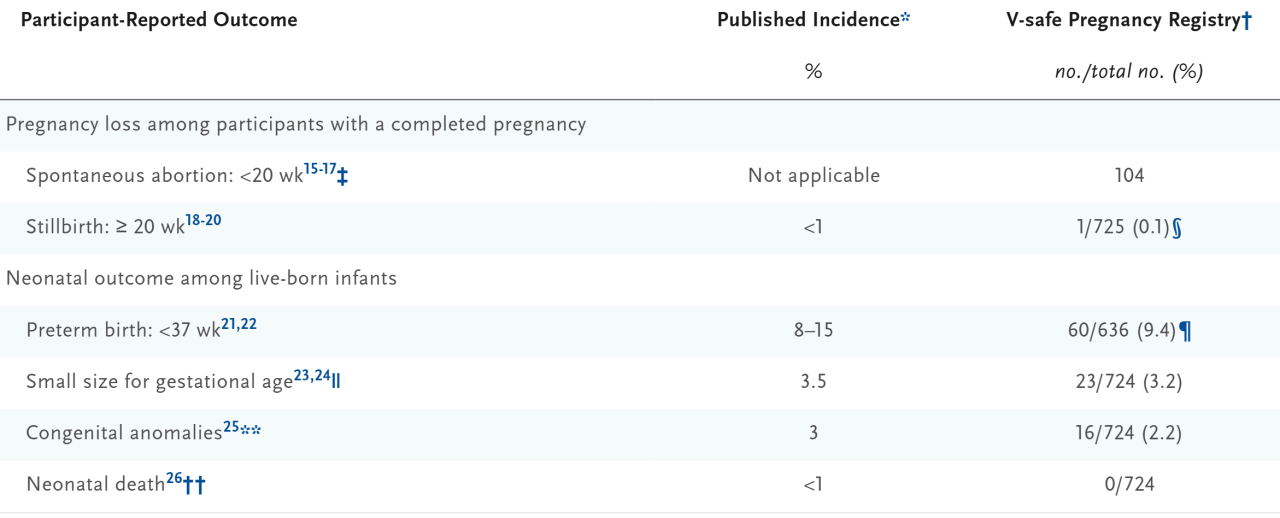
The V-Safe Women also did remarkably well with neonatal deaths. There was not one neonatal death, while with that number it would have been normal if three neonatal deaths had occurred.
4 keer zo weinig 'stillbirths'
In the general American population, fetal death is registered after 20 weeks of pregnancy as stillbirth With an incidence of approximately 0,57%6Official data: https://pubmed.ncbi.nlm.nih.gov/39832292/. In the V-Safe cohort, however, only 1 Stillbirth was reported on 827 (later corrected to 725) pregnancies, or 0,12%. (later 0.14%). That is 4 to 5 times less dan verwacht. Dit kan wijzen op onderrapportage. Vrouwen die een doodgeboorte meemaken, kunnen minder geneigd zijn een medische studie app als v-safe actief te blijven gebruiken. Emotionele belasting, rouw, of zelfs gevoelens van falen kunnen meespelen. Wie weet hebben er hun account gewist na zo'n late miskraam - we weten het niet.
Dat roept vragen op over de betrouwbaarheid van deze vorm van dataverzameling. De volledigheid van v-safe-gegevens hangt af van vrijwillige, actieve updates van deelnemers en van het te melden feit. Wie maakt zich druk om een app als zij net een overleden baby heeft gebaard... Gevoelige, pijnlijke, onwenselijke uitkomsten (mogelijk schuldgevoel bijvoorbeeld) worden ongetwijfeld minder graag gemeld dan neutrale of positieve zwangerschapsaflopen. De coöperatieve houding zal afnemen. Daarmee dreigt een systematische vertekening in de dataset - precies op de uitkomsten die voor een veiligheidsanalyse het meest relevant zijn. Zijn er meer afwijkingen in die richting?
No neonatal deaths
Er is in het onderzoek niet één melding gedaan van een baby die binnen de 28 dagen na de geboorte alsnog is overleden. Dat zal ook niet vaak voorkomen maar ik ben toch eens gaan kijken hoe vaak eigenlijk 'normaal' is. Dat blijkt in de VS bij de 3,5 per 1000 te liggen7Neo Infant Mortality in the United States National Vital Statitics Report Juli 2024, quite a lot actually. If you expect 3.5 then it is very unprecedently that there is no one among 800 women? Not impossible perhaps but very unlikely.
It is remarkable that two different negative pregnancy outcomes each show a deviation of 4–5 times lower than expected. Do we smell an elixir again?
It previously raises questions about the completeness of the report, about the usability of this data set and about the study (s) in which these questions have not been raised.
It will also be stated that the differences are not significant, but if that is not the case, what do the results actually show, given the uncertainty margins?
Hardly any abortions? Yes that is due to the sample!
The strikingly low number of reported induced abortions (abortion provocatus) also seems skewed. In the American population ends approximately 18% -20% of all pregnancies In an induced abortion8Guttmacher https://onlinelibrary.wiley.com/doi/10.1363/psrh.12215. However, there are only 10 Reported on the 827 included pregnancies (= all pregnancies with outcomes, of all cohorts). There are 15 to 20 times less Then expected.
It is striking that this discrepancy in the study itself remains undisputed. No explanation is given for the small number of abortions, nor referred to possible selection effects or sub-reporting. That is remarkable, because the difference is extremely large and a structural bias suggests. It suddenly seems obvious that we have to deal with deviating figures. Well, it would also say something about the reliability of the other findings.
Of moeten we toch, net als bij de andere data, concluderen dat vaccinaties helpen tegen abortus...? Dat is een sterk stuk. Maar er is wel een draai aan te geven.
We make a distinction between two types of induced abortion: therapeutic (medically necessary) and elective (At the request of the pregnant woman, for no medical reason). According to national figures, only 5–10% of all abortions are therapeutic. That is approximately 1.4% of all pregnancies. That would then correspond to the total number of abortions in the cohort.
Dan zou een hypothese kunnen zijn dat de vrouwen die ongewenst zwanger waren zich niet hebben aangemeld voor een langdurige medische follow-up, in dit geval v-safe. Dat hang je niet aan de grote klok, laat staan dat je het laat vastleggen - je hebt er nota bene anonieme klinieken voor of je moet het zelfs in een andere staat laten doen. Reden genoeg voor vrouwen die ongewenst zwanger werden en de optie overwogen om die zwangerschap af te breken, om zich niet in te schrijven. Waarom ook? Het is iets waar je niet graag mee te koop loopt en het voorspelbare verloop van jouw zwangerschap staat toch helemaal los van de vaccinatie...
Of het zo zat - we weten het niet. Maar alleen als we hiervan uitgaan, dat geen enkele ongewenst zwangere dat heeft gemeld in v-safe, of deelname heeft geweigerd bij ongewenste zwangerschap, of haar account heeft gewist bij ongewenste zwangerschap (wettelijk verplichte mogelijkheid), dan kloppen de abortus-cijfers weer een beetje: de geïnduceerde abortussen zijn dan uitsluitend medisch noodzakelijke ingrepen.
Er valt heel wat uit te leggen bij deze data, terwijl je toch zou hopen dat data juist verhelderend werken. Zeker als je ze als onderbouwing gebruikt. Dan moet het niet noodzakelijk zijn om ze eerst naar de verwachte cijfers toe te redeneren.
Also in discussions afterwards, Pro-Vaxxers also find the bias in the abortions of the research method of the research method, but the earlier positive outcomes really remain attributed to the vaccine, crooked sample or not. Whether that by -catch is put aside as not relevant: the vaccines are safe, point.
Summary
V-Safe does not offer a representative picture of all pregnancy outcomes. It shows women who want to propagate a pregnancy and are willing to share their medical process. Anyone who wants to make the questionable data should make assumptions: that only therapeutic abortions have been reported that people with a stillbirth may delete their account, and so on. But as soon as such assumptions become necessary to make data plausible, the scientific value of the dataset has already largely evaporated.
In short: the under-report of death births, neonatal death and induced abortions in the V-Safe cohort indicate structural limitations of this dataset. Because the data suggests that negative and/or medical outcomes are under-represented, this data set is pre-eminently unsuitable to serve as a reliable basis for safety conclusions on COVID-19 vaccination during pregnancy.
Why this analysis is still important
De publicatie van Shimabukuro et al. (NEJM, 2021) heeft een brede invloed gehad juist toen het erop aan kwam. Het was een strategisch ingezette boodschap, gebracht in het vertrouwen dat de toekomst het gelijk zou bewijzen. Het is bijna ondenkbaar dat de auteurs zelf tevreden waren met hun gammele onderbouwing. De onwaarschijnlijke data lijken wel authentiek. Daar wordt niet aan gemorreld want als datamanipulatie wordt ontdekt dan geldt dat als hard bewijs van datafraude. Men kijkt wel uit. De softere weg is dat data niet kunnen leiden tot gemaakte conclusies, want dat kan dat worden geduid als "verschil van wetenschappelijk inzicht; zo werkt wetenschap nu eenmaal".
The article was (and still) frequently quoted in systematic reviews and other studies, including publications in Vaccines (Basel), PLOS One, The Lancet Infectious Diseases and Frontiers. Policy authorities such as the CDC and FDA refer to their briefings and in formulating vaccine advice. International organizations such as the WHO and ECDC also took it into their safety communication.
Given this scientific and policy impact, critical evaluation remains of great importance. A reassessment of this basic data is necessary to draw reliable conclusions about the safety of COVID-19 vaccination during pregnancy.
This peer reviewed study is still online. In a broader context, it proves that scientific vaccine safety studies cannot simply be trusted. Even if they are performed by governments or by scientists with pharmaceutical tires.
1237 References in scientific articles
Google Scholar So far reports 1237 quotes and references to this study. A small handful question the methodology of the study, but the overwhelming majority sees it as support for one's own results. That is the consensus.
Then there are Systematic reviews, among others in The Lancet. Multiple major reviews evaluate the safety of COVID -13 vaccination in pregnant women. Shimabukuro window. Is referred to as a key study:
- The Lancet Infectious Diseases review: “These findings are consistent…”
- Frontiers studie: “CDC v-safe COVID‑19 Pregnancy Registry team has recently published preliminary findings…”
- PLOS One Systematic review: Underlines the Conensus
CDC & FDA documents
Reporting and policy letters about vaccine safety-such as FDA briefing documents from December 2020-refer to the Safety Registry data (including this V-Safe Data)
Public Health Ontario synopsis
Their summary (September 2021) discusses the V-Safe study extensively and notes some corrections and limitations that are not seen as serious impediment for the conclusions.
C-Span Interview Met Tom Shimabukuro
In a public C-Span interview9C-SPAN: Shinhibuma Special On America's public channel for parliamentary reporting and policy interviews bespreekt de hoofdonderzoeker de data zelf, wat aantoont hoe breed de methodologie als gezaghebbend werd aangenomen. De eerdere adviezen bleken dus goed gegokt, wat opgelucht en dankbaar werd omarmd in zijn studie - en natuurlijk vooral: geprezen in de media.
Footnotes
- 1
- 2
- 3
- 4The controversial study of Shimabukuro: https://www.nejm.org/doi/10.1056/NEJMoa2104983
- 5The controversial study of Shimabukuro https://www.nejm.org/doi/10.1056/NEJMoa2104983
- 6Official data: https://pubmed.ncbi.nlm.nih.gov/39832292/
- 7Neo Infant Mortality in the United States National Vital Statitics Report Juli 2024
- 8
- 9C-SPAN: Shinhibuma Special On America's public channel for parliamentary reporting and policy interviews

This post has been behind a password for a few weeks. Three readers thought that "not ok". Excuse for that!
Obviously accepted excuse. It's your site so you are the boss. I thought it was a shame and immediately looked in my e-mail if I had received a password, unfortunately not. Then I was looking for the statement by myself, it would come through my letter and/or not mention my name in the reactions ... Fortunately now that this good article can read and again very usable because family and acquaintances in Belgium. Says it on!
I was viewing your list of products that a pregnant woman is not allowed to take. Now the question arises, why are all those products not recommended that can cause a bacterium or virus infection?
Everyone who takes these products runs a chance of infection. Normally these bacteria/viruses are dead on our immune system.
And there light a crucial aspect. Why are pregnant women more comprehensible for such disorders?
As the pregnancy progresses, the unborn life suppresses the immune system of women. This is an interaction between child and mother to prevent rejecting the "not own meat", and therefore an early end of pregnancy.
It is therefore a very normal idea to protect pregnant women against an "unknown" virus, with a vaccine.
For the rest, your argument is completely correct. We are simply lying again with incomplete data/examinations.
I also don't say that pregnant women should not have a solid, monitored, safe vaccine?
That the warning for drop exists but you do inject an experimental genetically modified stuff that has never been tested for pregnant women (not even on pregnant laboratory animals), that is the point.
Zo bedoel ik het ook niet. Maar ik vind wel, dat de achtergrond ook duidelijk moet zijn. Waarom wil men graag zwangeren beschermen?!. En daar is mijn inziens een goede reden voor. Veel beter dan 12-17 jarigen.
Maar dan nog wil je niet alleen de moeder beschermen, maar ook het ongeboren leven. Maar aan het onderzoek te zien, waren daar ineens wat minder gegevens over bekend. M.a.w. ‘Eén pruts onderzoek”. Volkomen terecht dat je daar je meer dan terechte kant tekeningen bij plaats.
Anton, I assume you saw the interview with Leon Kuunders on BLCKBX. The way CIMS is set up is quite dramatic, but unfortunately quite standard when it comes to government IT projects. I see a 1 on 1 relationship with the conclusions that Master & Co have drawn.
I am familiar with large -scale IT projects. They usually go wrong, especially when it comes to the government. There are also always people who warn in advance and they are usually ignored.
Hugo knew this, but stopped the clean appearance. The system rattled on all sides, but also the entrance was not arranged, just like the Connceties with other relevant organizations such as Lareb.
For me this was (partially) new, but there were some puzzle pieces in place.
Especially seen and I also follow @leon1969 on X and we have contact occasionally. It's all true. Herman can also make it arithmetic, but it continues to sail in dense fog due to lack of (good) data.
That good data will never come I fear. Too much has already gone wrong.
The fact that the government has knowingly and knowingly the fiasco of failing registrations hid and continued with the mantra "safe and effective" has therefore actually been proven.
The intention was apparently originally to register any side effects, but that was never done seriously. The population (the majority at least :-)) is therefore consciously led to the garden.
Perhaps this fact should be the big spearhead of the criticism. You can indeed endlessly steggelen about the (partly missing) data, it will be a well -to -day welles/Nietes game. But the events about CIMS and the way in which this failure was consciously worked under the carpet leaves much less room for discussion. Without decent monitoring you can never maintain that the "vaccinations" have been a success. But yes, that "mysterious" excess mortality….
Exact. For people like Jan Bonte, Corona is pretty much over. He remains a doctor.
What matters of course is the system rot. It was not about Corona at all, it is about science corruption, false information, indoctrination, propaganda, data fraud and manipulation that have come to light in this "epidemic". And actually earlier, with the Mexican flu.
In a while another virus will come by, and they have another Wonderpanacee. It would be desirable to prevent a new catastrophe and to have solid monitoring in order. That really doesn't have to be that complicated - if the will is there.
Datalek (s) population screening and more. Big in the news now. Also not in order (again)? Or do we have to believe that everything in one system in the hands of the government (NATO) is the best ... Less fumbling is still done with less fumbling than in the Netherlands, little is still done in other countries to admit that there has been conscious system rot and still.
Ockham’s razer tegen een fictief narratief
Off topic, alhoewel.
Ook mensen werkend in de virologie en mRNA vaccin industrie hebben zo hun belangen met een eigen (fictief?) narratief en zijn niet blij, eerder doodsbenauwd voor deze niet angstig geworden, vaardige hanteerders van Ockhams razor.
https://odysee.com/$/download/The-Spike-Protein,-Dr.-Stefano-Scoglio/aabfa0a85dacc128c65a888527e48450d9ba436d
Vond hem via:
https://open.substack.com/pub/unbekoming/p/the-third-story-what-really-killed?utm_source=share&utm_medium=android&r=1lysl7
Het plaatje bij bovenaan deze site kan zo maar een exosoom zijn :-).
Ik had deze ook gezien. Scoglio zegt dus dat mRNA (via LNP’s) helemaal niet werkt. Niet werken kan en geeft daar een uitgebreide uitleg bij. Ik weet het even niet meer, ben zelf geen wetenschapper, geen medicus maar wel erg benieuwd wat men ons probeert aan te smeren. De werkelijkheid is waarschijnlijk weer nog complexer, en dat maakt het helemaal lastig als leek om ergens over de oordelen.
Je hebt dus mensen die
1. geloven in de heilzame werking van mRNA ‘vaccins’. Dat het immuunsysteem antistoffen aanmaakt op basis van de spike eiwitten die zich manifesteren op de celwand (of is het cel membraan?) en dat bijwerkingen ‘zeldzaa’zijn.
2. geloven dat de mRNA’s meer kwaad dan goed doen. De LNP’s gaan het hele lichaam door. spike eiwitten worden aangemaakt op plekken waar dat niet zou moeten. Ontstekingen ontstaan, gezonde cellen worden vernietigd, kortom chaos. Nog afgezien van foute celdelingen en vervuiling van de LNP’s tijdens productie. De ‘Inside mRNA’ film geeft hier ook een aardig beeld van.
3. En nu dus Coglio die beweert dat het mechanisme (met in LNP’s verpakt mRNA) helemaal niet kan werken. En hij geeft daar ogenschijnlijk zeer plausibele argumenten bij.
Heel lastig om hiertussen te navigeren. Optie 1 is een gepasseerd station, en ik neig naar 2. Maar kunnen we 3 zomaar uitsluiten en op welke gronden? Misschien eens iemand als Maarten Fornerod vragen.
Jan Bonte: Een arts met een groot hart EN op de goede plaats. Ik lees dat ook Jan van zijn stoel is gevallen door de uitzending bij blckbx met Leon Kuunders. Zo in de goede volgorde gezet is het verhaal duidelijker. Ook ik heb geprobeerd om het Lareb, de GGD’s en anderen te bevragen over de systemen die de veiligheid hadden moeten bewaken, velen vielen stil en dan hoopte ik dat het zaadje een beetje zou ontkiemen maar er waren er ook bij die schreeuwden “Neem die prik gewoon!”… Over corona praten is wat anders dan onderzoek doen, interesse in de echte cijfers, enz. kortom alles over de misstanden. Lees ook de Wuhan trilogie van Jan Bonte. Iedereen doet wat hij/zij kan, sommigen (Anton, Jan, Leon, en anderen) heel veel meer! Mijn helden!
Scherp Anton, de systeemrot is in alle essentiele zaken van een dusdanig niveau dat het ook steeds duidelijker wordt waarom dat CBDC er gewoon moet komen.
Want alleen naar het idee van maniakale giga falende bestuurders is totale controle de oplossing.
Wat dan doet denken aan het plakken van formule 1 banden met Duct-tape.
Nu het nog kan: kijk (en huiver) sam brok ken, dfacto punt nu, ook het week overzicht en d nieuwe wereld over privacy. Zelfs in mijn zeer kritische omgeving begint men camera’s (uit china) te gebruiken omdat het “van de verzekering zou moeten”. Je gaat niet met je tijd mee zeggen ze tegen mij. Waardoor ik mij geroepen voel om een “college” te geven over AI… maar het is geen wedstrijd dus probeer ik het allemaal los te laten. Uiteraard blijven er onderwerpen zoals “het echt beschermen van zwangeren” en “bijwerkingen en sterfte” waarmee we toch meer mensen over de streep kunnen trekken. 🤞
“Het is dus een hele normale gedachte om zwangere vrouwen juist te beschermen tegen een ‘onbekend’ virus, met een vaccin.”
Dit vind ik een hele domme, van Bonne Klok, nadat hij net heeft uitgelegd dat tijdens een zwangerschap het immuunsysteem van de vrouw verzwakt wordt. Vervolgens impliceert hij dus, in bovengeciteerde zin, dat een vaccin een virus buiten gevecht zou kunnen stellen, terwijl een kind zo langzamerhand weet dat een vaccin niet een virus bestrijdt, maar het immuunsysteem stimuleert tot verhoogde weerbaarheid tegen een virus, of andere ziekteverwekker, en dat immuunsysteem is nu net even niet in vorm, vanwege de zwangerschap. Kortom: wanlogica.
Zwangere vrouwen hebben per definitie iets in hun lichaam wat normaal gezien een afstoot reactie zou moeten veroorzaken.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3025805/
Ik heb te weinig kennis om alles te kunnen overzien.
Maar ik vraag me serieus af of de complexe balans in de baarmoeder van een zwangere vrouw iets is waar je zonder enig onderzoek goed advies in kan geven?