
The fact that Australia has not had Covid makes it an interesting case. Without an epidemic and with controlled lockdowns, there were never any problems with healthcare capacity. Long-Covid cannot explain excess mortality either. Wilson Sy (don't stop reading, because the flaw in his analysis is also discussed), an analyst with 62 publications, posted a Excess mortality analysis at Researchgate (25 pages) that in another article was discussed. Below is my version.
In the Netherlands, studies have been started that have to do with excess mortality. ZonMW, which approves or rejects the research proposals, is a VWS branch that has its task developed knowledge in the field of healthcare apply and stimulate research. The studies approved by ZonMW do not include studies that could be critical of possible personal or other medical failure. Medical malpractice is not mentioned as a possible dominant cause of excess mortality (think of vaccinations and measures). The main lightning rods are a) long Covid, b) delayed care and c) after-effects of (unnoticed) Covid - an idea suggested by Singapore. There too, they suffered from unexplained excess mortality after vaccination without having had a serious Covid epidemic.
In the first part of the study, Sy shows based on data from The Australian Bureau of Statistics (ABS) that there has been no Covid in Australia in 2020. What has happened to Covid mortality in that period is numerically not very relevant and can largely be attributed to false positive PCR tests. The minimal corona impact is also reflected on Ourwordlindata. Care capacity was no problem at all, hospital visits continued neatly by appointment.
After that, things get interesting. It is important to refer to the Bradford Hill criteria, which test the probability of causality in statistical correlation.
Correlation can become (almost) causality with the Bradford Hill test
There is a methodology to find causality in a correlation. For this purpose, the correlation must be tested against a number of criteria. There is discussion about how strong this causality actually becomes and whether there are any exceptions, but there is agreement that this 'checklist' is a valuable guideline. If all these criteria are met, there must be strong counterevidence. It is referenced a number of times. The enthusiast can open the bar below for more information.
De Bradford Hill criteria. Klik hier voor meer informatie.
| Strength (effect size): A small association does not mean that there is no causal effect, although the larger the association, the more likely it is to be causal. | Correlation coefficient of >75% |
| Consistence (reproducibility): Consistent findings observed by different individuals in different places with different samples reinforce the likelihood of an effect. | Observable at different times in most countries |
| Specificity: Causality is likely if there is a very specific population at a specific site and disease without any other probable explanation. The more specific an association between a factor and an effect is, the greater the chance of a causal relationship. [1] | There are no other candidates (in Australia) for the excess mortality, certainly not for the younger population. |
| Temporality: The effect must occur after the cause (and if there is an expected delay between the cause and the expected effect, then the effect must occur after that delay). | Zijn observaties signaleren de temporaliteit. (Model Steigstra reconstrueert oversterfteverloop zelfs puur op basis van temporaliteit.)
In Australië valt een 5-maanden vertraging op net zoals wij dat hier signaleerden.
 |
| Biological gradient (dose-response relationship): Greater exposure should generally lead to a greater incidence of the effect. However, in some cases, the mere presence of the factor can trigger the effect. In other cases, an inverse ratio is observed: greater exposure leads to a lower incidence. [1] | Number of doses determines the observed effects |
| Plausibility: A plausible mechanism between cause and effect is useful (but Hill noted that knowledge of the mechanism is limited by current knowledge). | So far, immunological, cardio-vascular and neurological effects of spike protein have been demonstrated. Multiple plausible mechanisms. |
| Cohesion: Coherentie tussen epidemiologische en laboratorium bevindingen verhoogt de waarschijnlijkheid van een effect. Hill merkte echter op dat "het ontbreken van dergelijk [laboratorium]bewijs het epidemiologische effect op associaties niet teniet kan doen". | Clinical trials do not contradict the long-term effects. Laboratory evidence is in line with the alarm signals from hotlines. |
| Experiment: "Af en toe is het mogelijk een beroep te doen op experimenteel bewijs". | Autopsies show causes of death from vaccinations |
| Analogy: The use of analogies or similarities between the observed association and other associations. | In the Netherlands: Swine Flu (passed by itself), previous misses with vaccinations |
| And candidate criterion: Reversibility: If the cause is removed, the short-term effect should also disappear. | The spikes in excess mortality have disappeared since no more campaigns are launched |
| These criteria are a work in progress. Adjustments have been proposed by a.o. Ioannidis and Shimonovich. | |
The iatrogenic epidemic from 2021 to 2023
De Australische oversterfte werd pas significant in 2021, net als bij ons de "onverklaarde oversterfte". Significante oversterfte was sterk gecorreleerd (+74%) met COVID-19 massale injecties vijf maanden eerder. Sterkte van de correlatie, consistentie, specificiteit, temporaliteit en dosis-responsrelatie zijn de belangrijkste criteria van Bradford Hill waaraan de gegevens voldoen om de iatrogenese (veroorzaakt door medisch ingrijpen) van de Australische epidemie te suggereren, waarbij de oversterfte grotendeels werd veroorzaakt door COVID-19-injecties.
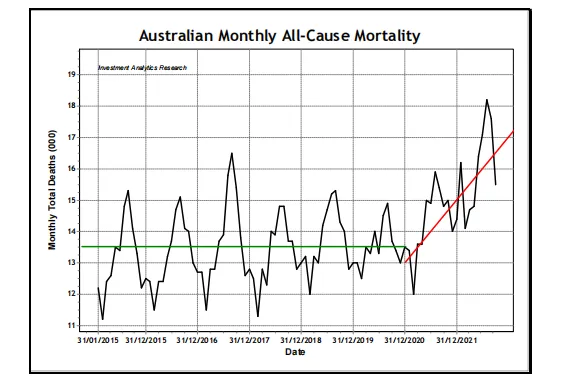
Figure 1: these are the last seven years. Each segment on the x-axis represents a year. The last segment before the red line is the year 2020. That year saw fewer deaths than the previous five years, so there was no 'pandemic' in Australia in 2020. The red line shows the sharp increase in the death rate - after the introduction of the Covid injections. So that is something to look at more closely.
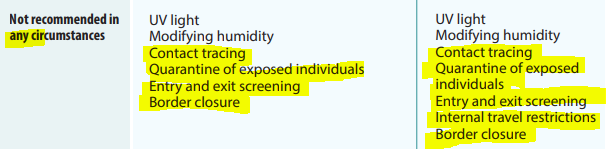
Before Covid appeared, there was a pandemic preparedness plan advising against lockdowns, masks and travel restrictions, advocating open borders but protecting vulnerable people. The logic was clear. Let the virus spread as quickly as possible among young and healthy people to achieve global herd immunity. A proven success story throughout evolution.
But this time, other forces intervened. The overly wrong modelling of Imperial College London caused panic and fear of overloading our hospitals. All preparedness plans, the thoughtful work of generations of scientists, were abandoned overnight. The rest is history.
After a year of draconian lockdowns and other restrictions, supported by military 5th generation psych-on warfare against their own people (see Robert W Malone MD, MS and Maajid Nawaz for detailed evidence), the new mRNA vaccines were the only state-sanctioned responses to the disproportionate threat of a Covid virus.
From March 2021 to September 2022, a period of one and a half years, more than 60 million doses of an unknown substance with very little data on efficiency and safety were injected into the arms of more than 20 million Australians. After that, about 60,000 more people died than expected. That's about 2,000 a month, an average of 24,000 a year. That is more than 20 times as much as the annual traffic victims. By comparison, Australia lost 34,000 soldiers during World War II. (Source) The injections doubled that total.
Waar het om gaat: hoe 'bewijst' Wilson Sy verder dat deze massale sterfte veroorzaakt wordt door de injecties? Hij toonde al een correlatie van 74% tussen injectie en dood. Dit is het sterkste criterium. Met betrekking tot de "Consistentie criteria" in de tijd biedt hij figuur 10 hieronder, Totale Doses vs Oversterfte aangepast door 5 maanden aanlooptijd.
The correlation is clearly visible. He also calculates a correlation of 31% when comparing other countries. It happens all over the world. The red line in this graph has shifted to the left for about 5 months.
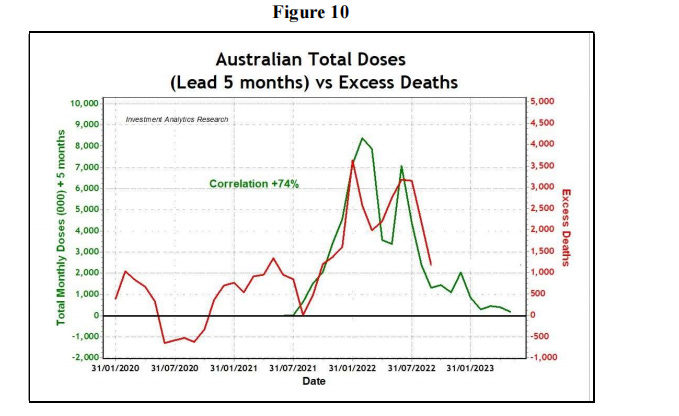
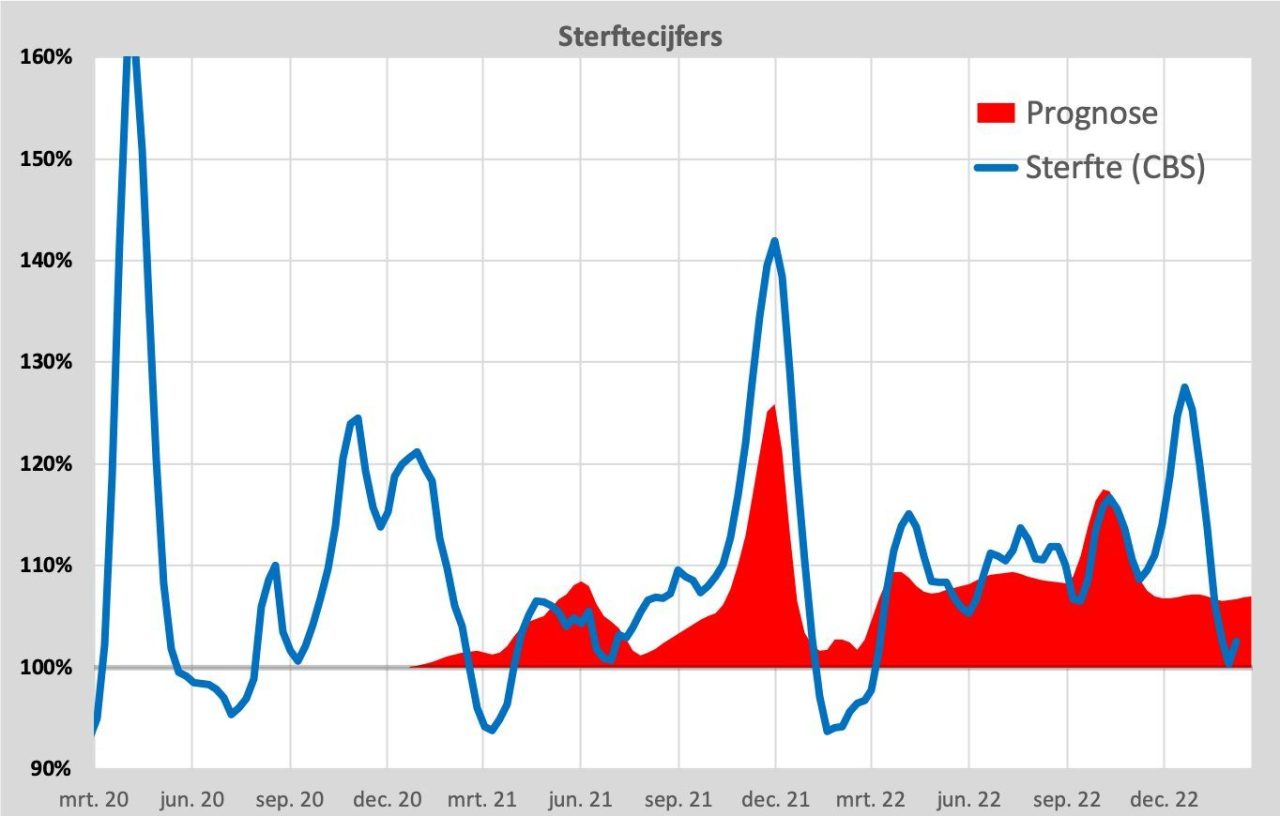
It is striking that the same five-month delay can also be seen in the Dutch excess mortality figures.

And if we are more sophisticated and we include both short- and possibly long-term effects, we can even simulate/prognotate the unexplained excess mortality fairly well. See the work of Herman Steigstra.
Specificity
Een ander nuttig criterium van Bradford Hill causaliteit is "specificiteit", dat verband houdt met de vraag of er concurrerende oorzaken zijn voor de oversterfte, met vergelijkbare associatiesterktes.
Correlation, even if consistent over time and in other countries, does not prove that there is primarily one cause. It becomes more specific by looking at the youngest age group. There are fewer possible confounding factors because the natural mortality there is very low. Despite the smaller number of additional deaths for the youngest age groups, the statistical signal is also present there.
In layman's terms: the elderly die from many causes. Young people hardly die and from very few causes. They also very rarely die from Covid itself, undermining speculation about Covid as a reason for an increased mortality rate.
Erratum - figures not reproducible
The text below sounded very convincing. Maurice de Hond pointed out to me that these figures are not in line with the historical data that we can download ourselves. Unfortunately, I hadn't looked that far when editing the article.
The text below does not seem to be correct, the percentages are considerably lower. Unverifiable numbers bolded:
"Wat statistisch zeer significant is, is dat de sterfte in de jongste groep van 0-44 jaar in 2022 ongeveer 160% is above historical expectations, while fluctuations for all age groups before 2022 are normally less than 20%.
The excess mortality for this age group in 2022 was consistently around 400 per month in Australia, meaning that in 2022 for each month "23-Sigma" cases occurred. This is an unprecedented statistical probability. It metaphorically means an earthquake of 9.5 on the Richter scale for epidemiology.
What other causes, aside from mass COVID shots, could meet Bradford Hill's basic criteria for Huge toename van sterfgevallen onder 44-minners te verklaren...?"
Coherence and plausibility
Wat de coherentie en plausibiliteit van Bradford Hill betreft: de suggestie van iatrogene oorsprong van overtollige sterfgevallen na vijf maanden na COVID-injecties is niet in tegenspraak met enig onderzoek naar "vaccinveiligheid". De uitgevoerde klinische proeven waren veel korter dan vijf maanden, meestal 11 weken. De gesuggereerde iatrogene oorzaak is in die zin coherent en niet in strijd met bekende feiten.
Are there plausible biological mechanisms that can explain the causal effect of COVID-19 injections on the excessive mortality of young and healthy people? Over the past three years, a deluge of research has been published on how the spike protein, either from the supposed SARS-CoV-2 virus infection or generated by the mRNA injections, could lead to inflammation in various organs that cause death. See This earlier article on this site.
Striking in Figure 1 is the seasonality, which could indicate immunological problems. For example, in a recently published clinical study of the mRNA injections observed that the production of neutralizing IgG3 antibodies against the spike protein switched over time to the production of non-neutralizing IgG4 antibodies. Is that related? Cardiovascular and neurological damage can also be expressed months later. Further research into the possible link with excess mortality should be the top priority.
Experiment and analogy
Om te beginnen wijst de auteur erop dat medische experimenten in Australië werden ontmoedigd om "vaccinatiebereidheid" niet in gevaar te brengen, ook niet als daar alle reden toe was. Ook werden postmortaal onderzoek en autopsies bepaald niet aangemoedigd.
For example, Australian doctors have been threatened with amounts of up to $20,000 for the use of serological tests to verify the results of the PCR tests for the diagnosis of COVID-19 (source). Niettemin is de wetenschappelijke noodzaak sterk genoeg om te hebben geleid tot verschillende post-mortem studies om het "smoking gun" bewijs van spike-eiwitten van COVID-injecties te ontdekken.
This is followed by a detailed, very specific discussion of the properties and behavior of spike proteins and related research. I refer to page 20 of the original PDF.
As an example of analogy, he refers to the swine flu pandemic:
Een analogie met de huidige COVID-19 pandemie is de "varkensgriep"-pandemie van 2009 als gevolg van het H1N1-griepvirus. Toen, net als nu, werd de pandemie niet op feiten gebaseerd, maar op verwachtingen van een zeer besmettelijke en zeer dodelijke ziekte die door de computermodellen van Oxford werd voorspeld. Het belangrijkste verschil is dat de "pandemie" van 2009 nooit tot een iatrogene pandemie kon worden omgevormd en dat zij snel vanzelf uitdoofde en uiteindelijk neerkwam op een zwakkere vorm van de seizoensgriep. De episode telde wereldwijd meer gevallen, maar minder doden (ongeveer 18.000) en een veel lager sterftecijfer dan de seizoensgriep (source). Volgens een definitie van oversterfte was het "Mexicaanse griep"-seizoen 2009 geen pandemie.
Conclusion
Based on mortality data, the Australian COVID-19 pandemic only began with the arrival of massive mRNA injections in 2021. It is ironic that mass injections, which were introduced to mitigate a non-existent pandemic, have caused a real iatrogenic pandemic. This study, including the Bradford Hill analysis, showed that injections administered to reduce pandemic mortality had the opposite effect, namely an increase in mortality.
The alarming excess mortality revealed by the data implies that the ratio of mortality risk to the benefits of COVID injections is very high, in a negative sense. That is, the damage or realized risk far outweighs the benefit of the COVID injections.

ZonMW is supposedly independent, but actually an extension of the Ministry of Health, because it is a 100% subsidy relationship. ZonMW will therefore never admit on its own initiative that the vaccinations are (the) cause of the excess mortality. ZonNet priori rejects research proposals into the cause of excess mortality, which include the vaccine policy.
Independent research via the regular (national) institutes or universities no longer exists in the Netherlands. Everything here is politicized.
... and multinationalized.
Is ZonMW an annex/ extension of the Ministry of Health, Welfare and Sport?
When I was still working at the Dutch Organisation for Scientific Research - and ZonMW was still called the Medical Sciences Area Board - all scientific research that was stimulated and subsidized there fell under the Ministry of Education, Culture and Science.
Nico, the government is increasingly working through external entities such as NGOs and foundations. This will have to do with data protection, liabilities and "independence". ZonMW is hanging on the drip of VWS, which is also on their website (in other terms of course). Their selection of approved studies gives the impression that they are simply an implementing body of VWS.
http://www.cobesitas.com. Resveratrol has been under investigation since April 2020. Peter van der Voort ic Groningen and member of the Senate d66 calls it a probabilistic remedy (recently said) but after his appearance at Jinek on 3 May 2020, he no longer tells that in public. On the mentioned website you can read that not everyone and certainly not healthy young people came to the ICU. Even after some clicking through on this website http://www.cobesitas.com it can be read that many ZoMw investigations are still not progressing or have just started, among other things. Children and the C-.
I also have my sources:-)
I had read the report before, but you explain it nicely, Anton. Thanks again!
What madness.
Then you were quick!
3 weeks before the election........well, you can think of that.
After the elections, excess mortality is attributed to a new pandemic, and then the "measures" come out of the toolbox
Hi Anton, you write that the period from March '21 to Sept '22 is two-and-a-half years, and then there is a whole calculation about the number of deaths. Very intense.
But the period from March '21 to September '22 is *one and a half* years. I don't know if that might make the math even more intense?
Corrected!
The figures mentioned are nothing short of shocking, not only for the vaccinated, but also for me as an unvaccinated person, because most people I know have been vaccinated.
The reason for not getting vaccinated was that they did not adhere to their own safety standards, did far too little research and introduced it hastily when there was objectively no need for it (there were medicines and the extra mortality was no higher than with a strong flu wave). You don't have to be an expert to see that the risks were irresponsible.
That evil dream of deaths due to vaccination now appears to be coming true, especially among young people who had nothing to fear from Corona.
Has anyone seen anything about this in the MSM?
Are they not looking at this site or would they rather keep it quiet again?
They're not watching. After a few lines, they qualify it as disinformation and dismiss it.
Do you already have access to the mortality figures including vaccination status in the Netherlands? Because I understand that they are public now.....
No, unfortunately still not.
Fast forward April 2025:
All links between the experimental mRNA injections and the enormous excess mortality and increase in serious diseases are still swept under the carpet.
Keep sharing this and other articles folks.
Many would otherwise not see the information, because they are too busy with their job and family in an increasingly expensive society.