
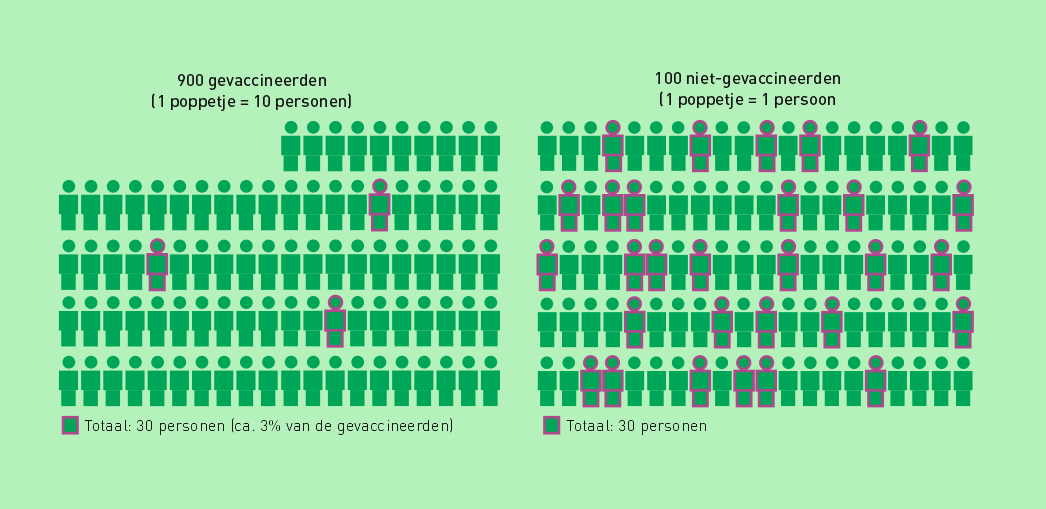
"In het huidige onderzoek werd ongeveer 3% van de ongevaccineerden eigenlijk wel gevaccineerd. Dit heeft waarschijnlijk geleid tot een onderschatting van de gevonden verschillen tussen gevaccineerden en ongevaccineerden" schrijft Nivel op pagina 38 van het oversterfterapport.
Nou, dat 'waarschijnlijk' kunnen ze wel weglaten of beter nog: vervangen door "Dit heeft geleid tot een enorme overwaardering van de vaccin-effectiviteit."
The curiosity about how effective the vaccines have really been has often led to all kinds of calculations by the RIVM and other institutes under the Ministry of Health, Welfare and Sport. They had (mostly secret) data and protocols that we have now also been able to view in part, thanks to the Meester/Jacobs report with the contributions of Bram Bakker and Wouter Aukema, later supplemented by @leon1969 who managed to retrieve the corresponding (Woo) documents.
The conclusion must be that the studies produced by our health institutes were rather pointless exercises, given the carelessness with which the data were collected and managed. And the same goes for the Nivel report.
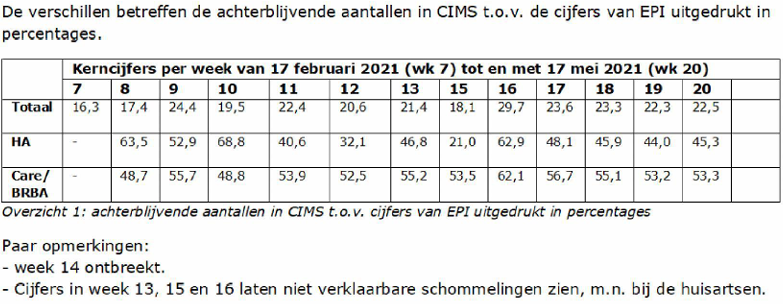
- The main stumbling block is that the vaccination statuses are not properly recorded.
There are periods of weeks of administrative backlogs, as a result of which a large number of deceased people (who died in those delay weeks between vaccination and status update) no longer appeared in the vaccination register when they had to be updated there. And so, with a jab, died and were removed from the registers before the registration of that jab could be processed. So died as unvaccinated. - There was also a ministerial regulation to remove deceased persons from the vaccination register, in order to keep track of the current vaccination rate. A column with 'date of death' could have sufficed, but the decision was made to delete the data.
- In addition, there are heavy healthy vaccinee and mortality depletion effects that, partly because of the registration problems, cannot be corrected. Especially in the first weeks/months after the jab, the vaccinated were therefore in much better shape than the group of unvaccinated people, which included people who were not vaccinated, precisely because of a short life horizon. In many studies, this advantage has served as the basis for the main conclusions, when it should have been corrected. (Science journalists don't seem to have the baggage to point this out. Again, hard evidence that the Fourth Estate is failing.)
Due to this accumulation of suboptimal carelessness, the vaccines are attributed too high an effectiveness. All unfortunate circumstances contribute to it. On the other hand, there are no flaws to be found that detracted from the effectiveness of the Covid vaccines. Things may change.
The Nivel workaround
To circumvent these problems, Nivel has estimated the chances of survival of both vaccinated and unvaccinated people based on health profiles and compares the observed mortality with this. No matter how carefully you do this, it's still guesswork. There is no guarantee that you have estimated the percent exactly. We'll see that every percent counts.
That's why registration is so meticulous. Nivel mentions a possible misclassification of 3%.
Now, at first glance, 3% seems like a fairly minimal estimate, @Leon1969 saw, flipping through Woo documents. Backlogs that amounted to several weeks, while a ministerial decree stipulated that deceased persons had to be removed from the register immediately. In other words, before the vaccination registration.

There is talk of 3% database anomalies, as if that would only affect the results for 3%. In reality, the deviations are many, many times larger (calculation now also on virus varia, by Herman Steigstra) but for now we are looking at that 3%. It has much more influence than 3% and I want to show that here. This is most clearly done with calculating vaccine effectiveness.
The Grateful Leverage of VE
A VE (vaccine effectiveness, in this case against dying) must be calculated using data from an RCT (Randomized Controlled Trial). An RCT is an investigation that must meet certain strict conditions. In retrospect, in a retrospective or observational study, those conditions are unachievable. I will highlight two of them here: Matching and Equal group sizes.
Matching means that ideally you have a comparable placebo subject for each subject. This is not the case after a vaccination campaign: the distinction between vaccinated and not vaccinated has already been made. This is almost always based on health characteristics and these will therefore influence the results when you look at your health after the injection. The Nivel report addressed this by estimating the chances of survival of vaccinated and unvaccinated subjects based on historical health profiles and comparing the injection results with them. Such an estimate already results in enormous uncertainty. A few percent off and in this case you are already completely wrong, as we will see.
Equal group sizes (a matter of course if you match well) are important because a death weighs equally in every group.
But with a vaccination rate of 90%, which is conceivable in a cohort of the elderly, one group is nine times larger than the other. That creates leverage with major consequences. I'll show you.
Suppose the vaccine has no effect: it is a placebo. Then you expect a result like this.
| Number | Deceased | SLEDGE (attack rate) | VE (ARo-ARg)/ARo x 100 | |
| Vaccinated | 900 | 90 | 10 | 0% |
| Unvaccinated | 100 | 10 | 10 |
But now it turns out that there is an administrative error somewhere: 3% of the vaccinated deceased are booked incorrectly. As a result, a number of vaccinated deceased people are booked as unvaccinated. So it's only about 2.7 out of 900 people!
As a result, the AR is indeed 3% lower in vaccinated people (from 10 to 9.7) but 27% higher in unvaccinated people (from 10 to 12.7)!
| Number | Deceased | SLEDGE (attack rate) | VE (ARo-ARg)/ARo x 100 | |
| Vaccinated | 900 | 87,3 | 9,7 | 24% |
| Unvaccinated | 100 | 12,7 | 12,7 |
So we get a placebo with a VE of 24% based on 3% misclassification.
With a misclassification of 10%, the VE of the placebo becomes 53%.
With a misclassification of 20%, the VE of the placebo becomes 71%.
With a misclassification of 40%, the VE of the placebo becomes 87%.
All this based on the somewhat exaggerated vaccination rate of 90%. The lower the vaccination coverage, the less strong the effect. But it is precisely in the older groups that vaccination coverage is highest, and that is precisely where the majority of deaths occur.
The thing is, it's terribly close.
In hoeverre dit fictieve cijfers blijven zal de toekomst hopelijk uitwijzen - dankzij Herman Steigstra of anders Maurice de Hond als die er nog mee aan het cijferen slaat. Sterker nog: Herman zit al te rekenen aan een reconstructie (link inmiddels gestuurd aan vv-subscribers, zie "Wanneer ben je gevaccineerd volgens CIMS").
No matter how you look at it, none of it fits with the excess mortality since the Covid jab frenzy.
Or maybe just...

0 Reactions