
This part 2 of the paper by Aseem Malhotra, I added afterwards to the post of Part 1, of September 26. That post became very long and early readers may have missed it. That's why I decided to write a separate article, also because there seems to be quite a bit of dust on it. In this part, the focus is on the failing system.
Below is the translation of Part 2
Part 2: A pandemic of misinformation
Wat met betrekking tot de vaccins tegen het coronavirus 2019 (COVID-19) duidelijk is geworden, is dat we te maken hebben met een pandemie van verkeerd geïnformeerde artsen en een verkeerd geïnformeerd en ongewild geschaad publiek. Het dwingend opleggen van deze COVID-19-vaccinaties (zeker geen op bewijs gebaseerd beleid) was een bijzonder flagrante misstap, vooral in het licht van duidelijke indicatoren die erop wijzen dat het gebruik van deze farmaceutische interventies - vooral in jongere leeftijdsgroepen - had moeten worden opgeschort. Een dergelijk beleid blijft de beginselen van ethisch evidence-based medische praktijk en geïnformeerde toestemming ondermijnen, ten koste van het optimaliseren van patiëntenresultaten.
In zijn paper uit 2017, 'How to survive the medical misinformation mess', benadrukken professor John Ioannidis en collega's dat:
Most clinical trial results are misleading or not helpful to patients. Most guidelines (on which many doctors rely to make treatment decisions) do not fully acknowledge the poor quality of the data on which they are based. Most medical stories in the mass media do not meet criteria for accuracy, and in many stories, the benefits are exaggerated and the disadvantages are minimized.1 (p. 1).
Een senior arts die regelmatig contact heeft met de Chief Medical Officer van het Verenigd Koninkrijk (VK), professor Chris Whitty, heeft onlangs tegenover mij zijn bezorgdheid geuit over het feit dat hij denkt dat de meeste van zijn collega's in leidinggevende posities die het gezondheidsbeleid beïnvloeden, het bewijsmateriaal niet kritisch beoordelen en in plaats daarvan vertrouwen op mediaverhalen over COVID-19 en het vaccin. Dit komt overeen met de bekentenis van Rochelle Walensky, de voormalige voorzitter van de Centers of Disease Control (CDC), wiens optimisme over de doeltreffendheid van het COVID-19 vaccin van Pfizer voortkwam uit het lezen van een CNN nieuwsbericht, dat een bijna letterlijke weergave was van het eigen persbericht van Pfizer.2
Has the British Chief Medical Officer Professor Chris Whitty critically assessed the evidence? Recently, he publicly shared a letter3 waarin hij aangaf hoe belangrijk het is dat gezondheidswerkers zich laten vaccineren tegen COVID-19. Deze brief was niet volledig en strookte niet met het totale bewijsmateriaal: "De COVID-19 vaccins zijn veilig en effectief". Het zou juister zijn geweest te stellen dat "het vaccin niet volledig veilig is en lang niet zo effectief als we hadden gehoopt. Niet eens in dezelfde buurt als de doeltreffendheid en veiligheid van traditionele vaccins".
Professor Chirs Witty stated:
Onze professionele verantwoordelijkheid is om de covaccins te krijgen zoals aanbevolen om onze patiënten te beschermen".3
Hij had moeten zeggen dat wat omicron betreft "het vaccin weinig tot geen bescherming biedt tegen infectie". Uit gegevens over de delta-variant blijkt ook dat er, eenmaal besmet, geen significant verschil is in overdrachtspercentages tussen gevaccineerden en niet-gevaccineerden.
De verklaringen van professor Whitty zijn vooral verrassend omdat de CEO van Pfizer heeft verklaard dat in verband met omicron "we weten dat de twee doses van een vaccin zeer beperkte bescherming bieden, als er al bescherming is".5
Could it be that Professor Whitty is also a victim of medical misinformation?
There are four main motivations and seven sins that underlie the medical misinformation:
Motives:
- Much published medical research is not reliable or is uncertain, does not benefit patients or is not useful to decision-makers;
- Most health professionals are unaware of this problem;
- Even if they are aware of this problem, most health professionals lack the skills necessary to assess the reliability and usefulness of medical evidence; and
- Patients and families often lack relevant, accurate medical evidence and expert guidance at the time of medical decision-making.1
Sins:
- Bidental research funding (that is, research funded because it is likely to be profitable and not beneficial to patients).
- tendentious reporting in medical journals
- tendentious media coverage
- Biased patient leaflets
- Commercial conflicts of interest
- Defensive medicine
- The inability of doctors to understand and communicate health statistics.6
Ioannidis en collega's benadrukken dat:
"De onwetendheid over dit probleem, zelfs op de hoogste niveaus van academisch en klinisch leiderschap, is diepgaand"1.
Samengevoegd over meerdere decennia hebben deze upstream en downstream risicofactoren voor verkeerde informatie een verwoestend effect gehad op de gezondheidszorg waarin we ons nu bevinden. Het teveel voorschrijven van geneesmiddelen wordt als zo'n bedreiging voor de volksgezondheid beschouwd dat twee vooraanstaande medische tijdschriften in de afgelopen 10 jaar (de BMJ en JAMA Internal Medicine) campagnes hebben gelanceerd om de schade van te veel medisch ingrijpen te beperken.
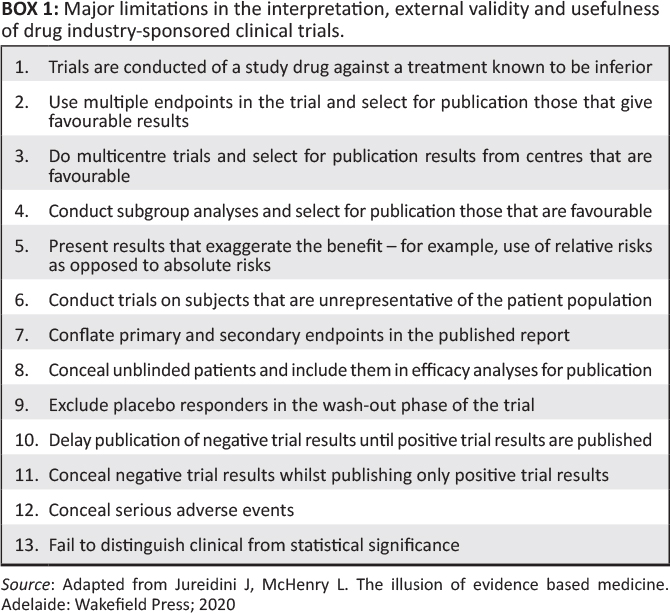
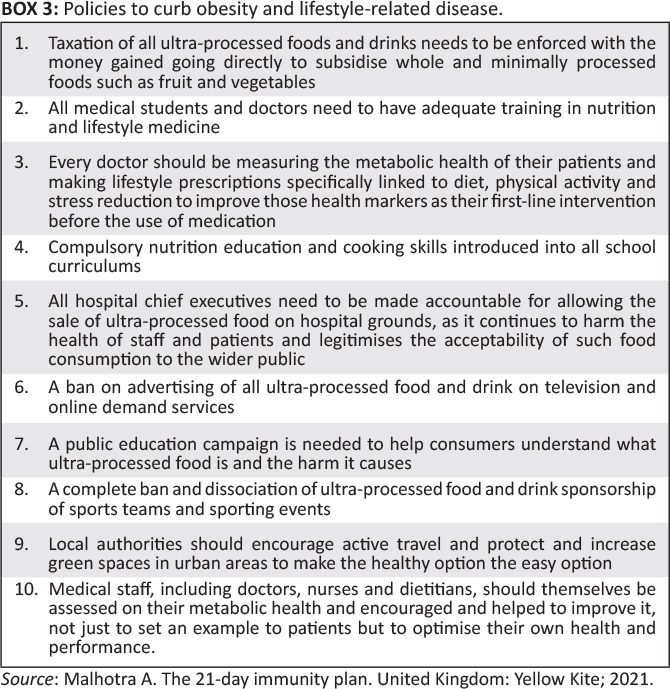
According to the co-founder of the Cochrane Collaboration, Peter Gøtzsche, prescription drugs are the third leading cause of death worldwide, after heart disease and cancer.7 This is not surprising when one realizes that most of the published research is misleading, especially when the benefits of drug research are exaggerated and the adverse effects of too many drugs are underestimated. (Box 18).
If a doctor makes clinical decisions based on biased information, it leads (at best) to suboptimal outcomes and (more worryingly) to harm to the patient.
Shortcomings of the medical profession
Volgens professor Carl Heneghan, huisarts in de spoedeisende hulp en directeur van het Centre of Evidence-Based Medicine van de Universiteit van Oxford: "bij elke ingreep die je als arts doet, moet je jezelf twee vragen stellen: hoeveel verschil maakt het? Hoe weet ik dat?"9
Building on the Academy of Medical Royal Colleges' Choosing Wisely campaign,10 it is instructive to note that in 2020 the General Medical Council issued guidelines on the duty of physicians to engage in shared decision-making with patients, underpinned by informed consent.11
Er zijn zes essentiële onderdelen van geïnformeerde besluitvorming: (1) beschrijving van de aard van de beslissing; (2) bespreking van alternatieven; (3) bespreking van risico's en voordelen (in absolute termen); (4) bespreking van gerelateerde onzekerheden; (5) beoordeling van het begrip van de patiënt; en (6) uitlokken van de voorkeur van de patiënt.
If the vaccine has not been administered in accordance with these principles (which is likely to be done on a large scale, in accordance with historical data)12)), dan is dit ook een aanzienlijke schending van de plichten van een arts van de General Medical Council om "patiënten de informatie te geven die zij willen of nodig hebben op een manier die zij kunnen begrijpen".13
It is instructive to note that the greater the financial interests in a particular field, the less likely it is that the research results will be true.14 As already demonstrated in Part 115 van dit artikel, heeft het verplicht stellen van een nieuw vaccin voor noodgebruik aan niet-kwetsbare mensen weinig tot geen effect op het voorkomen van infectie en ernstige ziekte, heeft het daarom geen wetenschappelijke geldigheid en schendt het daarom de beginselen van geïnformeerde toestemming. Het verhoogt echter de winst van de fabrikant enorm. Door het gebruik van het mRNA-vaccin uit te breiden tot de meerderheid van de bevolking die een zeer laag risico loopt op ernstige complicaties van COVID-19, maar meer kans heeft op ernstige en/of levensbedreigende bijwerkingen zoals myocarditis of plotselinge hartdood, heeft Pfizer tot nu toe tientallen miljarden dollars aan inkomsten gegenereerd, waardoor het een van de meest lucratieve producten in de geschiedenis is. Als beleidsmakers zich meer hadden gericht op het beschermen van de kwetsbaren - en artsen de kans hadden gekregen om samen met patiënten beslissingen te nemen op basis van transparante communicatie over risico's en voordelen - zouden de resultaten voor patiënten waarschijnlijk aanzienlijk zijn verbeterd,16 maar zouden de winsten van de farmaceutische bedrijven waarschijnlijk een fractie zijn geweest van wat ze feitelijk hebben opgebracht. Zoals voormalig redacteur van de New England Journal of Medicine Dr. Marcia Angell al eerder opmerkte: "de echte strijd in de gezondheidszorg is er een van waarheid versus geld".17
Institutional corruption and erosion of public trust
Institutional corruption is defined as the deviation of an institution from a baseline of integrity.18 There is a long documented history (both through studies and lawsuits) of the strategies by which drug companies hide, ignore, or misrepresent evidence about new drugs. Distortion of the medical literature and misrepresentation of data by companies looking to expand the market for their product can lead to over-prescribing, with the predictable result that millions of patients suffer from preventable side effects.
Vóór 2020 bestonden er al grove tekortkomingen in het medisch-industrieel complex - er was te veel invloed van de farmaceutische industrie op de klinische besluitvorming. Dit is niet onopgemerkt gebleven, met als gevolg een groeiende vertrouwenscrisis in medisch onderzoek: uit een rapport van de Academy of Medical Sciences in 2017 bleek dat 82% van de huisartsen en 63% van het publiek niet geloofde dat de resultaten van door de farmaceutische industrie gesponsord onderzoek onbevooroordeeld waren.19Also, only 37% of the public trust medical research, compared to 65% who trust the experience of their friends and family.20
Dit groeiende gebrek aan vertrouwen - onlangs nog verergerd door dwang, vaccinpaspoorten en weinig aandacht in de reguliere media voor een ongekende schaal van gerapporteerde schade aan vaccins onder de bevolking - werd onlangs geïllustreerd door de weigering van 8 miljoen mensen in het VK om de COVID-19 boostervaccinatie te nemen. Bovendien leidt alle aandacht voor COVID-19 (dat in zijn huidige omicronvorm vrijwel geen risico voor kinderen inhoudt) de aandacht af van, en zelfs erger nog, doet de verdenking rijzen op meer doeltreffende en veilige interventies zoals het mazelen-, bof- en rodehondvaccin (MMR). In het Verenigd Koninkrijk heeft de MMR-vaccinatiegraad de laagste stand in tien jaar bereikt.
Regulatory failures and investigative misconduct
De autoriteiten willen dat het publiek "de wetenschap vertrouwt", maar vaccinfabrikanten hebben met succes afspraken gemaakt met verschillende grote regeringen over de hele wereld die hen vrijwaren van financiële aansprakelijkheid in het geval van vaccin-gerelateerde schade. Interessant genoeg weigerde India, de grootste democratie ter wereld, Pfizer vrijwaring van schade voor zijn vaccin. Een Indiase regeringsbron vertelde Reuters dat:
The whole problem with Pfizer is the indemnification. Why should we sign it? If something happens, a patient dies, we can't question them [Pfizer]. If someone files a lawsuit, the central government is responsible for everything, not the company.21(p. 1)
Pfizer preferred to leave the Indian market rather than conduct a local safety and immunity study.22
It's important to first understand that drug companies have a fiduciary duty to make a profit for their shareholders, not a legal responsibility to give you the best treatment. During a lecture at the Centre of Evidence-Based Medicine in Oxford in 2014, Peter Wilmshurst said that the real scandal is that many of those with a responsibility for patients and scientific integrity (doctors, academic institutions and medical journals) often collude with the industry for financial gain.23 It is precisely this industry that has been found guilty of the most egregious corporate crimes: between 2003 and 2016, the 11 largest pharmaceutical companies paid $28.8 billion in fines in the United States (US) alone,24 many of them for criminal activities such as illegally marketing medicines, manipulating results and hiding data on harm. As noted in the BMJ, no systematic changes have been made since then to mitigate this damage.9
In an international survey of respondents from higher education institutions, 14% admitted to knowing a colleague who fabricated, falsified, and altered data, and 34% of scientists reported questionable research practices, including selective reporting of clinical outcomes in published research and the concealment of conflicts of interest.25 Een flagrant gedocumenteerd geval van wangedrag bij onderzoek betrof een prominente Nederlandse arts wiens werk van invloed was op de richtlijnen van de Europese Vereniging voor Cardiologie over het gebruik van bètablokkers bij niet-hartchirurgie. Hij werd ontslagen van de Erasmus Universiteit wegens "schendingen van de academische integriteit", waaronder het gebruik van "fictieve gegevens" in het onderzoek. Geschat wordt dat deze richtlijnen het sterftecijfer van patiënten met 27% hebben verhoogd, wat resulteerde in 800 000 extra sterfgevallen in Europa over een periode van 8 jaar.26
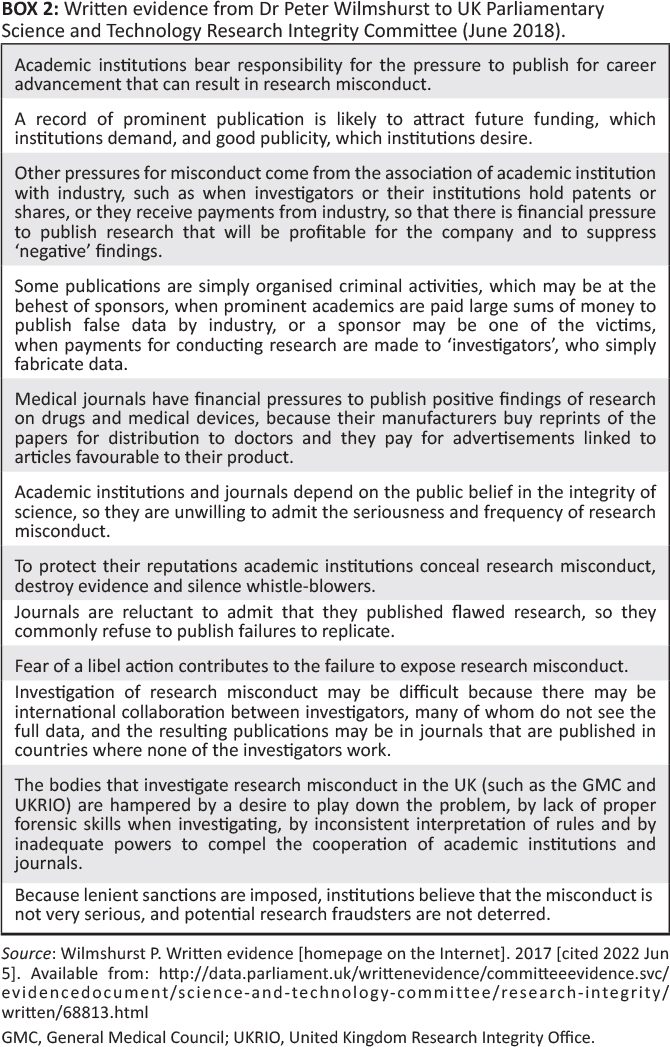
In evidence submitted in 2017 to the UK Parliamentary Committee for the Evaluation of Science and Technology on Research Integrity (chaired by Sir Norman Lamb), Dr Peter Wilmshurst lists a number of risk factors that encourage misconduct in research in UK institutions (see Box 2 27). His solution, which I agree with, would be to ensure that serious forms of investigative abuse are criminalized with meaningful sanctions and that allegations of such activities are investigated by an independent body with legal powers.27
A researcher from a prestigious British institution contacted me to inform me that in his cardiology department, a group of academics deliberately suppressed research showing that the mRNA vaccine significantly increased coronary risk, as determined by cardiac imaging, compared to the unvaccinated. The chairman of the group expressed concern that publication of the data could lead to a loss of funding by the pharmaceutical industry.28 After alluding to this in GB News, the whistleblower informed me that letters of non-disclosure had been sent to all members of the team involved in this particular area of investigation.
Evidence-based medicine and the rollout of the COVID-19 vaccine
Neither the drug authorities nor the vaccine manufacturers have yet shared all the raw data from the pivotal trials for the COVID-19 vaccines.29De ruwe gegevens van de klinische proeven omvatten duizenden pagina's die nog moeten worden vrijgegeven voor onafhankelijk onderzoek. Dit is belangrijk omdat in het verleden onafhankelijke onderzoekers die soms toegang kregen tot deze gegevens, de conclusies van de gepubliceerde proeven volledig onderuit konden halen: Een voorbeeld hiervan is Tamiflu.30Gaining access to clinical case reports for Tamiflu eventually revealed that the drug was no more effective than acetaminophen for flu and that it also had minor but significant drawbacks. The British government had stockpiled half a billion dollars for a drug that turned out to be useless, despite claims by the manufacturers (Roche, Basil, Switzerland) that it shortened the duration and severity of the disease. The independent researchers who were able to analyze the data concluded that all industry-sponsored research should be considered marketing until proven otherwise.
It is against this backdrop that transparency advocates have sued the Food and Drug Administration (FDA) to access the data on the basis of which Pfizer's vaccine (BNT162b2) was granted emergency use authorization.31 The FDA wanted a U.S. federal judge to give the agency 55 years to release this data.32 Waarom zou de FDA - "die verantwoordelijk is voor het toezicht op meer dan 2,7 biljoen dollar in de consumptie van voedsel, medische producten en tabak’33 - dit doen? Geheimhouding zou nooit een interventie op het gebied van de volksgezondheid mogen afschermen. De advocaat die optrad namens de eiser Aaron Siri meldde dat:
The government also tried to delay the full release of the data it relied on to authorize this product until nearly every American alive today is dead. This form of government is destructive to freedom and is at odds with the openness that is required in a democratic society.31
Instead, the judge ordered the FDA to release the data over an eight-month period after all commercially sensitive information had been redacted.
A major risk factor for failing to protect the public from such harm is the lack of independence of the regulator. The FDA's Center for Drug Evaluation Research (CDER) receives 65% of its funding from the pharmaceutical industry (primarily in the form of user fees).34 For example, as part of the approval process for its COVID-19 vaccine, Pfizer made in May 202135 a transfer to the FDA of $2,875,842 under the Prescription Drug User Fee Act of 1992.36Full FDA approval for Pfizer's COVID-19 injection followed in August 2021.37, despite recent evidence that the original RCT data indicated a greater risk of serious adverse reactions to the vaccine than to hospitalisation due to COVID-19.
Afzonderlijke analyses hebben aangetoond dat de overgrote meerderheid van de nieuwe geneesmiddelen die de afgelopen decennia door de FDA zijn goedgekeurd, later slechts kopieën van oude geneesmiddelen bleken te zijn, wat niet verwonderlijk is als men beseft dat geneesmiddelenbedrijven 19 keer meer uitgeven aan marketing dan aan onderzoek naar nieuwe moleculaire entiteiten, wat allemaal bijdraagt tot aanzienlijke verspilling. Tussen 2000 en 2008 bleek slechts 11% van de 667 door de FDA goedgekeurde geneesmiddelen echt innovatief te zijn. In de VS wordt geschat dat 30% tot 50% van de gezondheidszorgactiviteiten geen voordeel oplevert voor de patiënten. Uit een onderzoek onder wetenschappers van de FDA bleek dat 70% van hen vond dat de FDA niet over de middelen beschikte om haar missie "de volksgezondheid te beschermen … en het publiek te helpen nauwkeurige, wetenschappelijk onderbouwde informatie te krijgen om geneesmiddelen en voedingsmiddelen te gebruiken om hun gezondheid te verbeteren" effectief uit te voeren.38
Een analyse van elk nieuw geneesmiddel dat tussen 2002 en 2011 in Frankrijk werd goedgekeurd, toonde aan dat slechts 8% enig voordeel bood en dat het dubbele daarvan - 15,6% - schadelijker dan heilzaam bleek te zijn, terwijl de meerderheid van de andere nieuwe geneesmiddelen in wezen kopieën van oude geneesmiddelen waren en bijdroegen aan een kolossale verspilling van overheidsgeld.18Similar conclusions have been drawn in Canada and the Netherlands. In my view, the evidence is overwhelming that the overall net effect of the pharmaceutical industry on society and public health over the past few decades has been very negative.
COVID-19 vaccination in persons at lower risk
Regardless of the benefits of inoculating higher-risk groups, where a small but significant benefit may exist against the original Wuhan strain, inoculating lower-risk children in the name of preventing asymptomatic transmission does not have strong scientific validity and therefore exposes them to potential harm.
In the United Kingdom, the Office for National Statistics has disclosed an as yet unexplained significant increase in deaths among 15- to 19-year-old children since May 2021 compared to the five-year average. Has the COVID-19 vaccine been ruled out as a possible cause, given what we now know about potential harm, especially with regard to myocarditis, myocardial infarction, and sudden cardiac death (even in 16- to 39-year-olds)?39
In September 2021, the Joint Committee on Vaccination and Immunisation (JCVI) issued a controversial recommendation that the Pfizer/BioNTech vaccine is marginally beneficial for 12- to 15-year-old children.40The Medicines and Healthcare products Regulatory Agency (MHRA, the UK equivalent of the FDA) had previously stated that:
Zij hebben de klinische studiegegevens van het Pfizer/BioNtech-vaccin bij meer dan 2.000 kinderen van 12-15 jaar zorgvuldig bestudeerd en zijn tot de conclusie gekomen dat de voordelen van dit vaccin opwegen tegen de risico's en dat het effectief en aanvaardbaar veilig is in deze leeftijdsgroep […] Er werden geen nieuwe bijwerkingen vastgesteld en de veiligheidsgegevens bij kinderen waren vergelijkbaar met die van jonge volwassenen. Net als in de leeftijdsgroep van jonge volwassenen waren de meeste bijwerkingen licht tot matig en hielden ze verband met reactogeniciteit (bv. pijnlijke arm en vermoeidheid).41(p. 1)
Is this in line with the overall evidence?
Award-winning investigative journalist Maryanne Demasi published the harrowing story of one of the trial participants, 12-year-old Maddie De Garay. After severe abdominal pain followed by seizures, she was admitted to the hospital and now she is permanently disabled, wheelchair-bound and fed via a nasogastric tube. In Pfizer's study, they reported her side effect as mild: stomach upset.42
Het is belangrijk te benadrukken dat het risico van overlijden door COVID-19 bij een 12- tot 15-jarige bijna nul is, namelijk 1 op 76.000. In overeenstemming met de beginselen van ethische, op bewijsmateriaal gebaseerde medische praktijk door middel van gedeelde besluitvorming, moet de ouders worden verteld dat er geen gegevens van hoge kwaliteit zijn waaruit blijkt dat het vaccin bij kinderen infectie, overdracht, ernstige ziekte of overlijden voorkomt, maar dat het ernstige bijwerkingen kan hebben zoals myocarditis - vooral bij jonge mannen, waar het voorkomt bij 1 op 270043 - en ernstige invaliditeit.
Can financial interests influence the recommendations?
Op haar website verklaart de MHRA dat het merendeel van haar financiering afkomstig is van de farmaceutische industrie en 3 miljoen pond (Britse ponden) van de Bill and Melinda Gates Foundation (BMGF). Zijn beleidsmakers en het publiek ervan op de hoogte dat het aandelenkapitaal van de stichting zwaar belegd is in voedingsmiddelen (waaronder McDonald's en Coca-Cola) en farmaceutische bedrijven, direct en indirect? Zoals in een Lancet-paper uit 2009 wordt opgemerkt, worden de prioriteiten van de financiers vaak bepaald door persoonlijke belangen en niet door de prioritaire gezondheidsbelangen van het ontvangende land.44 "De portefeuille van de BMGF met farmaceutische bedrijven verdient aandacht gezien het persoonlijke geloof van de heer Gates in de rol van octrooien als motor voor innovatie op het gebied van geneesmiddelen en medische technologie".45
Obesity researcher Dr Zoe Harcombe has also examined the financial ties that may influence the position of the Joint Committee on Vaccines and Immunisation and found that the members of the subcommittee work for organisations that receive a total of $1 billion from the BMGF.46 It is also worth noting that Professor Wei Shen Lim, Chair of the JCVI Subcommittee on Vaccines, is directly responsible for the material funding his department receives from Pfizer.47 This in no way suggests that the JCVI has acted incorrectly, but when trust in an organisation such as the JCVI is necessary, it is essential that there is no perception of conflicts of interest. The systems for selecting panelists, examining evidence, and the methodology and openness of their recommendations must be impeccable.
The most direct cause of harmful health outcomes: Corporate power and the commercial determinants of health
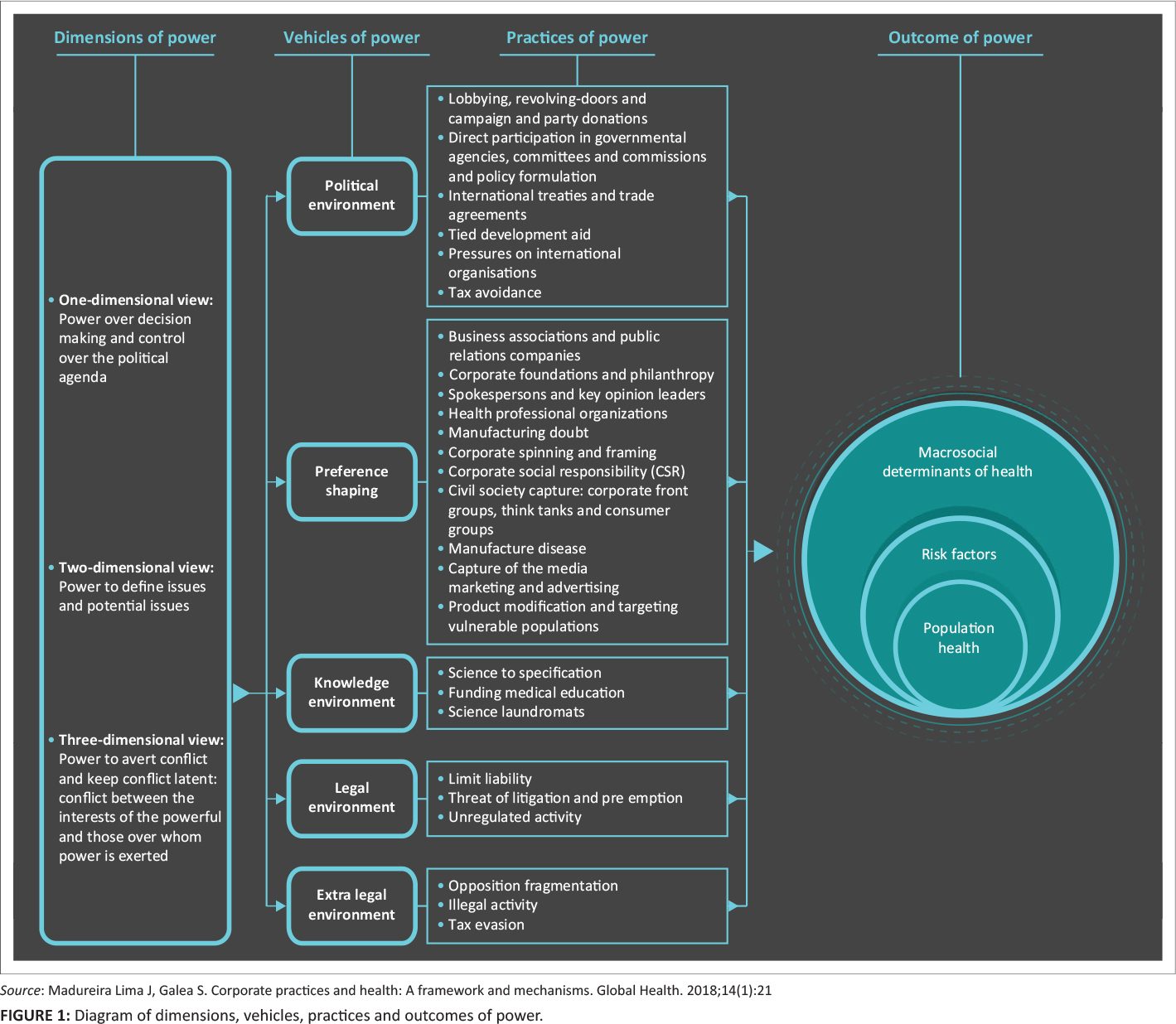
De commerciële gezondheidsdeterminanten kunnen het best worden gedefinieerd als "strategieën en benaderingen van de particuliere sector om producten en keuzes te promoten die schadelijk zijn voor de gezondheid".48Corporations exercise their power through a combination of factors, including intellectual exploitation. This includes the ability to determine the dominant narrative, establish the rules and procedures by which society is governed, determine the rights, living and working conditions of ordinary people, and appropriate knowledge and ideas49 (see figure 145).
In the case of the mRNA vaccine, Pfizer seems to have benefited at least to some extent from this corporate framework strategy by shaping the knowledge environment (Pfizer was responsible for the design and conduct of the trial, the data collection, the data analysis, the data interpretation and the writing of the manuscript), the political environment (lobbying), the formation of preferences (corporate foundations and philanthropy, spokespersons and key opinion leaders, influencing the media), the legal environment (limitation of liability) and the extra-legal environment (fragmentation of the opposition by removing critics of the current dominant narrative that the vaccine is safe and effective).45
As a result, it has earned tens of billions of dollars from a product that is extremely ineffective compared to proven traditional vaccines and most other drugs and contains unprecedented reports of serious harm.
Distorted media coverage and censorship of legitimate scientific debate
Companies are able to form preferences and shape the dominant narratives about the determinants of health, through unchecked invisible power. One way is to own mass media. The global media market is dominated by seven companies and chains that own 80% of the newspapers in the US.50 De subsidies van het BMGF aan wereldwijde mediabedrijven zijn opmerkelijk - zo heeft The Guardian Media Group de afgelopen 12 jaar meer dan 12 miljoen dollar aan subsidies van het BMGF ontvangen. De controle over reclame in de gedrukte en uitgezonden media heeft ook invloed op redactionele beslissingen. De meeste gezondheidsjournalisten (waaronder een aantal die ik heb gesproken) zijn zich er over het algemeen niet van bewust dat de informatie die zij voor hun verhalen verkrijgen bewust is vormgegeven door de particuliere belangen van fabrikanten en "onderzoeks"universiteiten.
De BBC, hoewel schijnbaar niet direct beïnvloed door industriële belangen, wordt door sommigen traditioneel gezien als de meest betrouwbare mediabron in het Verenigd Koninkrijk. Haar berichtgeving over kwesties rond COVID-19 is naar mijn mening (mogelijk door extra druk van de regering) uiterst slecht geweest en - specifiek over kwesties rond het vaccin - schromelijk onzorgvuldig. Tijdens een recente reportage over tennisser Novak Djokovic die zijn besluit toelichtte om het vaccin niet te nemen tot hij meer informatie heeft over de voordelen en nadelen ervan, stelde een verslaggever de vraag "hoeveel meer informatie heeft hij nodig?". De verslaggever verzuimde te vermelden dat Djokovic COVID-19 heeft gehad en dat er aanwijzingen zijn dat natuurlijke immuniteit aanzienlijke bescherming biedt tegen herinfectie en ernstige ziekte, en dat systemische bijwerkingen bijna driemaal zo waarschijnlijk zijn bij mensen met natuurlijke immuniteit die vervolgens worden gevaccineerd.
Verder heeft de BBC ten onrechte een gast van de populaire podcasthost Joe Rogan, Dr. Robert Malone, afgeschilderd als een "bekende anti-vaxxer, die tegen het vaccineren van kinderen is", zonder te vermelden dat Dr. Malone mede-uitvinder is van de technologie die tot het vaccin heeft geleid, 20 jaar werkzaam is geweest bij de ontwikkeling van vaccins op het niveau van de Amerikaanse overheid en een van de eersten was die daadwerkelijk twee injecties met de Moderna jab heeft gekregen. De BBC verzuimde ook vreemd genoeg een van de belangrijkste verhalen over de pandemie te publiceren in een van de meest gerespecteerde en invloedrijke medische tijdschriften ter wereld: Een onderzoek door de BMJ bracht bewijzen aan het licht van slechte praktijken bij een contractonderzoeksbedrijf dat betrokken was bij Pfizer's cruciale COVID-19 vaccin onderzoek. Een regionale directeur van een van de proeflocaties in Texas, VS, documenteerde bewijzen dat Pfizer gegevens vervalste, patiënten niet blindeerde, inadequaat gecontroleerde vaccinatoren tewerkstelde en traag was met het opvolgen van bijwerkingen. Dezelfde dag dat ze haar klacht naar de FDA e-mailde, werd ze ontslagen.51 She then filed a fraud lawsuit against Pfizer on behalf of the U.S. government (and the people of the U.S.) under whistleblower law. Pfizer's motion to dismiss the case (which apparently failed to convince the judge) was based on the fact that the FDA had not responded to its (or other) complaints, so the allegations were of no concern to the government.
In de VS zei senator Ron Johnson, die hoorzittingen hield met gezondheidswerkers die gegevens presenteerden over duidelijke, substantiële en zeer veel voorkomende bijwerkingen van de mRNA-prikken, die brede publieke aandacht verdienden, dat "de reguliere media medesamenzweerders zijn in deze politieke vuile truc. Zullen zij ter verantwoording worden geroepen voor hun rol in dit bedrog?"52
Sociale mediaplatforms blijven schuldig aan het verspreiden van desinformatie. Door hun bedrijfsmodel, dat gericht is op het koste wat kost vergroten van de betrokkenheid, verliest de samenleving steeds meer toegang tot de waarheid en verslechtert ons vermogen tot empathie als individu, waardoor nog meer verdeeldheid en vijandigheid wordt gezaaid. De zogenaamde "fact checkers" hebben alles gecensureerd wat het heersende mainstream verhaal (de gevestigde orde is betrouwbaar en de vaccins zijn volkomen veilig) in twijfel trekt. Ze bestempelden zelfs het onderzoek van het BMJ naar mogelijke fraude in de cruciale proef van Pfizer als desinformatie en stopten gebruikers het verhaal te delen op hun platform. In een brief van de huidige en voormalige hoofdredacteur van het tijdschrift aan Mark Zuckerberg wordt de integriteit van Facebooks feitencontroleurs in twijfel getrokken:
Rather than investing a proportion of Meta's substantial profits to help ensure the accuracy of medical information shared through social media, you apparently delegated responsibility to people incompetent in carrying out this crucial task.53(p. 1)
It has also come to light that Facebook has partnered with drug company Merck to decide what content to censor on its platform in relation to COVID-19 and the vaccine.54 Is Facebook aware that Merck has paid one of the largest fines in U.S. history for being found guilty of fraud related to their painkiller Vioxx?55 Not only did one study find that the drug did not reduce stomach bleeding (their original main selling point) compared to ibuprofen, but it also significantly increased the risk of heart attacks and strokes, causing an estimated 40,000 to 60,000 additional deaths over a five-year period.56
Improving metabolic health
The lack of public health messaging and policies to help people improve their lifestyles during the pandemic is a missed opportunity to mitigate the harms of respiratory diseases like COVID-19. After age, obesity and conditions related to excess body fat are the biggest risk factor for worse COVID-19 outcomes. More than 90% of deaths from COVID-19 occurred in countries where more than 50% of the population is overweight or obese. The United Kingdom's biobank data during the first wave showed a more than four times higher risk of hospitalization due to COVID-19, depending on lifestyle factors. For example, a non-smoking adult in their mid-50s with a normal body mass index (BMI) and adequate exercise had a 1 in 1,521 chance of being hospitalized after contracting COVID-19, while an obese, smoking, sedentary person's risk was 1 in 327.57
The hypothesized pathophysiological mechanisms of the risk and complications of an infection include a series of markers that cause insulin resistance and chronic inflammation.
Even a single high blood glucose reading in non-diabetics (a marker of insulin resistance) who are hospitalized has been found to be associated with worse outcomes.58
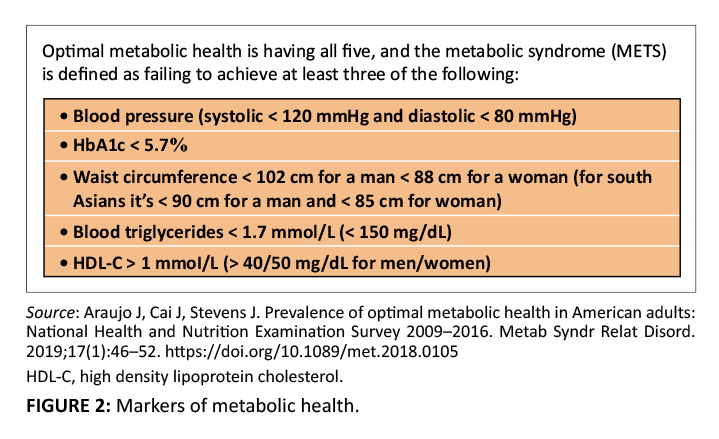
Recently, it has also been found that in the UK, of the 175,256 deaths associated with COVID-19 (2020-2021), less than 10% (17,371) had COVID-19 as the sole cause on the death certificate, suggesting that the risk of COVID-19 for individuals with optimal metabolic health (Figure 259) was significantly smaller, according to the results of the above-mentioned UK biobank study.60
De overheid en de medische autoriteiten hadden prioriteit moeten geven aan het benadrukken van het belang van het elimineren van ultraverwerkte voedingsmiddelen en koolhydraten van lage kwaliteit om het risico te verminderen. Ze hadden het publiek erop kunnen wijzen dat is aangetoond dat de omkering van het metabool syndroom bij tot 50% van de patiënten - onafhankelijk van gewichtsverlies - binnen vier weken kan optreden door alleen het dieet te veranderen.61
The coronavirus disease 2019 was a short-lived crisis that took advantage of a slow pandemic of poor metabolic health (see Figure 259), which is also the main cause of the major chronic diseases that have been putting increasing pressure on healthcare systems around the world for decades. It is estimated that a healthier lifestyle (in absolute terms) could eliminate 40% of cancer cases and 75% of cases of cardiovascular disease and type 2 diabetes.63
Optimal metabolic health would not only improve the immune system's resistance, but also reduce the burden of heart disease, type 2 diabetes, cancer, and dementia.
Learning lessons from tobacco control: policy changes addressing the availability, acceptability and affordability of highly processed foods and beverages and low-quality carbohydrates would significantly reduce the burden of obesity and related metabolic diseases and are likely to optimise the population's immune resistance within a few years (see Box 362).
The solutions
Er was nooit enig bewijs dat COVID-19 vaccinatiemandaten, paspoorten of een van de andere dwangmaatregelen van verschillende regeringen wereldwijd rechtvaardigde. Elke patiënt die een COVID-19 vaccin aangeboden kreeg, had moeten weten wat zijn risico op COVID-19 is, afhankelijk van leeftijd en risicofactoren. In overeenstemming met een ethische medische praktijk hadden de artsen de patiënten moeten meedelen dat hun absolute risicovermindering voor besmetting met de vorige, dodelijker variant ongeveer 0,84% of 1 op 119 bedraagt (gebaseerd op niet-transparante gegevens) en dat dit beschermingsniveau slechts enkele maanden duurt. Zij hadden ook nauwkeuriger en degelijker gegevens moeten verstrekken over wat de werkelijke absolute individuele risicovermindering van COVID-19-dood door het vaccin is, wat de werkelijke percentages van ernstige bijwerkingen (zoals blijvende invaliditeit, ziekenhuisopname of overlijden) zijn. Alleen wanneer artsen en patiënten over al deze informatie beschikken, kunnen zij in staat worden gesteld om openhartige gesprekken te voeren over de vraag of een behandeling - met inbegrip van dit vaccin - voor hen de juiste is.
The profession should explain that optimizing metabolic health gives patients the best chance to ensure that they are not only resistant to infection, but also reduce their risk of chronic diseases such as heart disease, cancer and dementia.
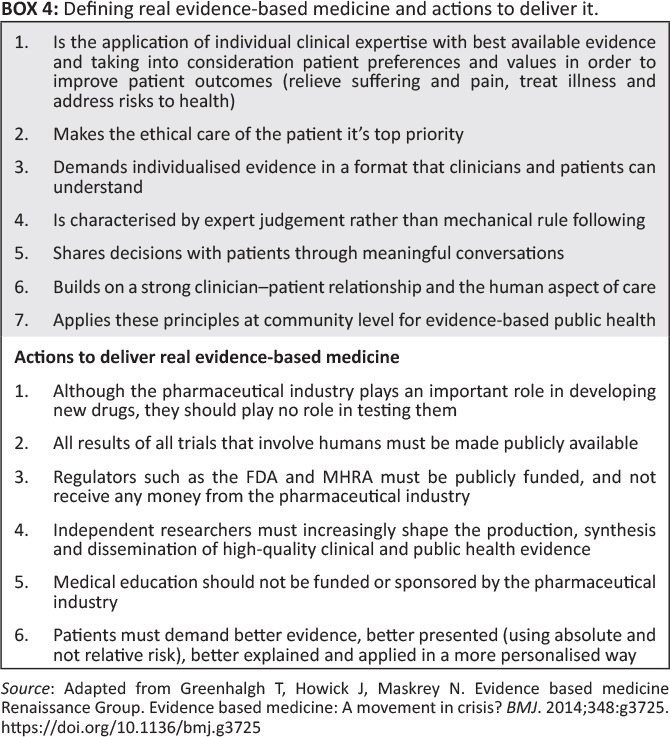
The time has come to prevent misleading evidence from entering the media and clinical decision-making and resulting in unethical and unscientific policy decisions. It is time for real evidence-based medicine (Box 464).
There are also strong scientific, ethical, and moral arguments for halting the current administration of the mRNA vaccine until Pfizer releases all raw data for independent research.30This will provide a more accurate picture of the groups that are more likely to benefit from the vaccine than the groups that are more likely to be harmed.
Gezien alle recente goed gedocumenteerde bovengenoemde tekortkomingen in de integriteit van medisch onderzoek (waaronder dat mogelijk de helft van de gepubliceerde medische literatuur 'gewoon onwaar kan zijn'), schreef de redacteur van de Lancet Richard Horton in 2015 dat de wetenschap een wending naar de duisternis heeft genomen en vroeg hij wie de eerste stap ging zetten in het opschonen van het systeem.65 The unprecedented rollout of an emergency use vaccine without access to the raw data, with mounting evidence of significant harms, exacerbated by mandates that seem to serve no purpose other than to support drug industry profits, have exposed the worst failings of modern medicine on an epic scale, with additional catastrophic damage to public health confidence.
We should use this as an opportunity to transform the system into better doctors, better decision-making, healthier patients and restoring confidence in medicine and public health. Until all raw data on the mRNA COVID-19 vaccines have been independently analyzed, claims that they provide a net benefit to humanity cannot be considered evidence-based.
Credits
I thank Dr. Clare Craig for edits and data analysis, and Alex Starling for comments and suggestions. The author is also grateful for the help of a scientist who wishes to remain anonymous due to career pressure.
Competing interests
The authors state that they have no financial or personal relationships that could have inappropriately influenced them in the writing of this article.
Author's contribution
A.M. is the sole author of this article.
Ethical considerations
This article followed all ethical standards for research without direct contact with human or animal subjects.
Financing information
This study did not receive a specific grant from a funding agency in the public, commercial or non-profit sector.
Data availability
Data sharing does not apply to this article, as no new data was created or analyzed in this study.
Disclaimer
The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of any body affiliated with the author.
Again the link to Part 2

What a TOP article, the crowning glory of your work Anton! It will have taken you many hours and days to produce this, thank you very much for all your efforts!
I only translated it. That was a bit of work, but not days! We owe the real work to Dr. Aseem Malhotra.
Off topic, but perhaps interesting for visitors of this site: a lecture by a British professor of statistics for whom I already had strong admiration before Covid and who has remained just as rational as Anton.
https://media.ed.ac.uk/media/1_k4ksrgbr
Fantastic!!! The ease with which that man talks you through those formulas... And then the discussion at the end, great. The statistics are way over my head. But jazz sometimes does that too and yet you can hear whether it is right or not. Enjoy!