
Even with absurdly high doses, scientists were unable to get test subjects to get Covid with the original SARS-CoV-2 virus. The researchers recommend that even higher doses and older subjects should be considered in future studies. It would also help if the subjects hadn't already gone through the disease, they say. However, those people are no longer to be found. A major scientific problem for future research into Covid vaccines.
In response to the article "Scientists Tried To Give People COVID – And Failed" in Nature, 1 May 2024. Study Here.
Purpose of the study
It was not an experiment to demonstrate the power of natural immunity. Nor was our first and most important line of defense, mucosal immunity, tested. No, here's the thing: the assessment of a vaccine requires a standardized infection model (a "CHIM"). It describes the exact method of how to infect test subjects. Of course, if this is done in different ways in studies, it makes the results incomparable. According to the scientists, the only important factor is the administered dose of the virus.
They therefore want future corona vaccines to be able to be tested thoroughly and in a standardized way. In the past, this has not been necessary (regulations are devised for this and definitions are revised), but people in virologists' land are happy to do so. And besides: there appears to be an inexhaustible pot of money in the corona sector.
The virus in question was the original SARS-CoV-2 virus. Why such an outdated variant...? "Maybe they should get off those vaccines," my ever-practical wife suggested. And indeed: There may still be millions of those vaccines in Ursula's basement or else on the phone on which the text messages with repeat orders were received. Then it helps to be able to show cheering research results, for which you simply need test subjects. But without sick people, that becomes difficult.
 And what do you mean 'future corona vaccines', that's ready now, isn't it? Well, no: in England, for example, the age limit for the target group with weakened immune systems is just Reduced to 6 months. It is still thought that dysfunctional immune systems respond well to the corona vaccines. And they apparently also think that a vaccination in May still offers protection in the next flu season, which may not present itself for six months... And then with outdated vaccines too. That is going to be disappointing again => another reason to urgently booster by then!
And what do you mean 'future corona vaccines', that's ready now, isn't it? Well, no: in England, for example, the age limit for the target group with weakened immune systems is just Reduced to 6 months. It is still thought that dysfunctional immune systems respond well to the corona vaccines. And they apparently also think that a vaccination in May still offers protection in the next flu season, which may not present itself for six months... And then with outdated vaccines too. That is going to be disappointing again => another reason to urgently booster by then!
Reinfection in case of natural immunity
In a previous similar study, almost half of the subjects were successfully infected with a dose of 1×101 (TCID50) pre-alpha SARS-CoV-2 virus (take it for granted. Just note that 101, which is 10 to the power of 1). But by then, the virus hadn't circulated yet! The researchers realized that the situation has changed: almost everyone has now been in contact with the virus and has built up natural immunity.
What do you do then? Well, that follows the same logic for these people as that of the vaccines: if one vaccination doesn't work, more vaccine is needed, so you do a double shot. If that still doesn't work, then apparently more vaccine is needed because vaccine works. So there has to be a booster after it. Etcetera.
From this point of view, it is only consistent that the researchers expected that they would be able to higher dose of the same virus the test subjects would still get sick.
Note: the same virus that those test subjects were once infected with, the 2019 version.
Would these top scientists also think that, if you have had the measles well, you can still get measles again? As my wife rightly pointed out, "Anyone who has had measles themselves and has cared for children with measles knows that this is nonsense."
It works very differently with measles than with a rapidly mutating virus. You can get the latter again as soon as it has mutated sufficiently, and especially if you have been vaccinated against an older strain. There is even more to covid vaccination: the more corona vaccinations you have had, the greater the chance that you will become infected. See, at least, the earlier Cleveland study And there is also a New preprint ready that gives the same picture.
Note: My mother taught Hygiene and Infection Prevention to nurses. She may not have been very familiar with microbiology or virology, but she knew everything about hygiene, disinfection, contamination risks, infection, airing rooms, transmission, sterilization, infection treatment, etc. Higher up in the medical hierarchy, that profession is no longer considered interesting: "We have nurses for that." They prefer to focus on cell cultures and titers. This is noticeable, also when it comes to the transmission route, about which more later.
How did vaccinated people perform?
An intermediate question. Unvaccinated test subjects also participated in this "CHIMS study". Everyone had had Covid, including the vaccinated. It is apparently completely normal that there are hordes of vaccinated people who have still had Covid. That penny certainly didn't drop with the researchers.
Unfortunately, due to the distribution of the test subjects among different groups, it is impossible to say anything about the performance of the vaccinated compared to the unvaccinated. A missed opportunity or rather: a missed opportunity, because it is not a coincidence.
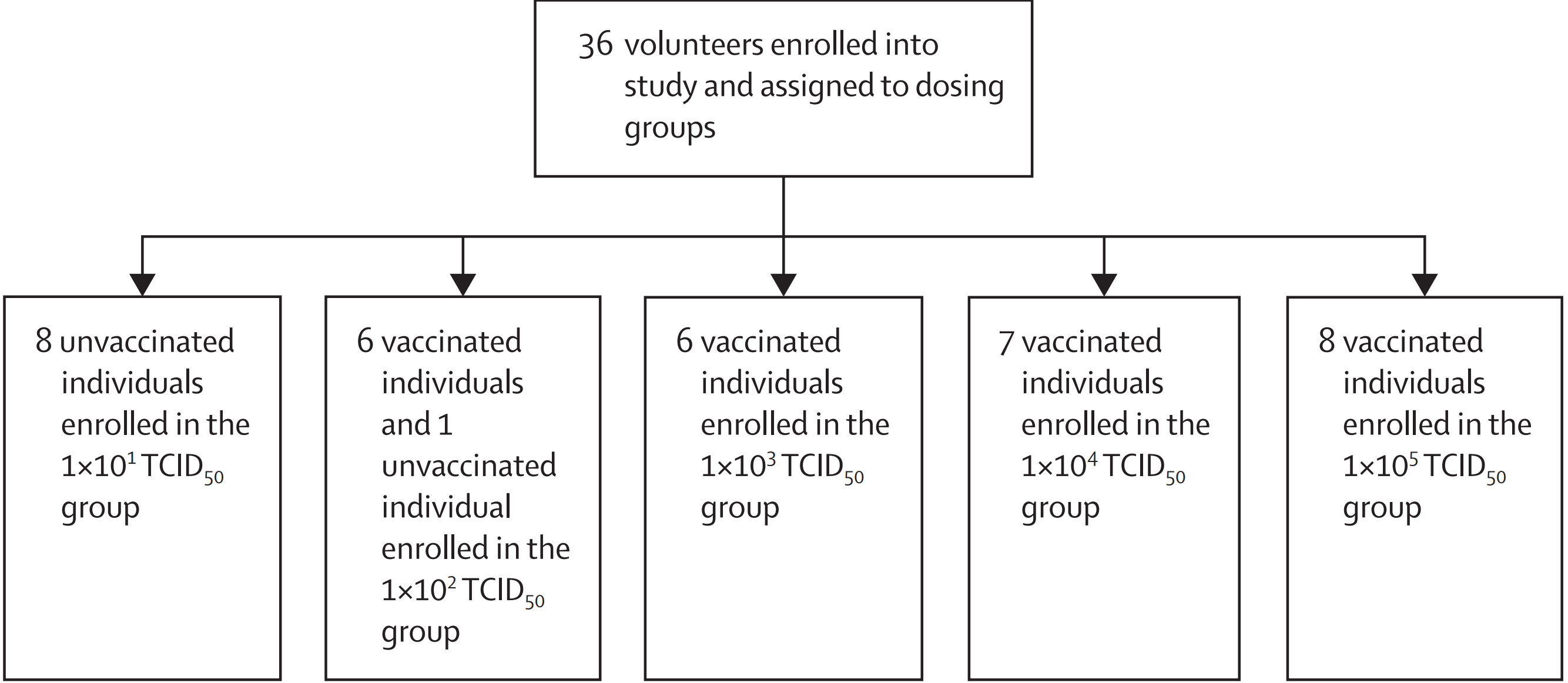
Subjects are divided into 5 groups, inoculated by 1×101, 1×102, 1×103, 1×104 and 1×105tcid50SARS-CoV-2. With the increase of each power, a zero is added, so 1×105 is a 10,000x higher dose than 1×101. Somewhere in between, one expected an effect.
All but one of the unvaccinated have been strategically grouped together in the group with the lowest dose. At least: it can't be a coincidence because that chance is about 1 in 3 million, I checked that with the help of chatgpt 😅. What could have been the motive for this? The researchers state that they had started by recruiting only unvaccinated subjects, but due to the ever-increasing vaccination rate, this was no longer possible after 9 candidates. Then they also started admitting vaccinated people. So they filled the containers chronologically, I understand. I think it's a strong piece.
At first I thought it might have been for ethical reasons: "those poor unvaccinated people were the least protected so it was irresponsible to expose them to a high dose"... That is not a very convincing argument because the same dose had been used in previous research and there were no accidents. And those subjects hadn't even been immunized yet.
Chronologically, with the side effect that no comparison is now possible between vaccinated and unvaccinated people. If the unvaccinated perform worse, it is of course because they were never vaccinated. In the unlikely event that they perform better, this could be explained by the fact that they had had the lowest dose.
Had made three groups of 12, each with 3 unvaccinated people in it. Then you would have had at least something of a control group in each group. The study could then have shown, for example, that in each subgroup only the unvaccinated became ill, which could have been useful as well. It is a pity that they have ruled out that possibility in advance. But then again, that's not what the study was about.
In the end, it didn't matter: it just didn't work to make me sick. Even with a 10,000 times higher dose, they were unable to induce long COVID infection in the volunteers, none of them. A stuffy nose here and there, that was about it. There was a lot of swabing and PCR testing but no.... They signaled some elevated levels from time to time, but it all went away pretty quickly.
Fun fact
The subjects were followed for 12 months. In that period, Mother Nature did it for a while: 39%(!) of the test subjects spontaneously experienced a new Covid infection during that period. That's a lot: 14 out of 36. One of the test subjects even twice! I'm so curious about his vaccination status...
The scientists do not elaborate on this either, except that they note that it was Omicron. 14 pieces, that could not have been only the unvaccinated. After all, there were only 9 of them. So at least 5 were vaccinated. Maybe more, 7, or 10. That would then be an indication that the vaccinations offer little to no protection against later variants, at least since Omicron.
Or would that entire 39% have consisted of only vaccinated people and the unvaccinated remained out of harm's way of Mother Nature? Would that be reported? I didn't see anything about it.
You can find a definite answer about this in the follow-up post. The link is at the bottom of this article.
PCR test: no association
Incidentally, the study mentions that infections are measured with a PCR test. Virus and vaccine research is of course impossible without a specific PCR test. I have pointed it out before, but I will take the opportunity again: the Wuhan lab was a leading center of research with corona viruses. However, our virologists did not get our PCR test from there. They also did not make any use of the knowledge that was available there at the time when a virus broke out in that very region.
On the contrary, they managed to make that PCR test super fast based on messages in social media. So there is no association there. That's just, yes, not an association.
Solutions to the problem
At the end, in 'Discussion', the brainiacs recommend that in similar research not only healthy volunteers between the ages of 18 and 30 should be taken. Including the elderly increases the risk of disease, they suspect. And they give the tip to dose at 1×107 (i.e. 1 million times higher as the aforementioned reference study. 1,000,000x stronger! They are really distraught. And something of insight is starting to ripen because their advice is not to take the original virus anymore but a later variant:
The use of Prevalent Variants would be more relevant for the evaluation of vaccines and therapies and work is underway to use variants known to demonstrate immune escape, such as Delta (ISRCTN94747181) or Omicron.
So they have found out that it is not very useful to do research on variants that no longer exist and to which everyone is immune. Boy. Progressive insight, shall we say.
And even then, what are the prevalent variants now? Does anyone remember why we stopped naming after Omicron? That was because nothing more happened. Of course there is still some numbering, but the Name Branding Has left much to be desired since Omicron. So this experiment actually shows that natural immunity protects well and that the later, spontaneously contracted, variants no longer cause significant damage.
So there goes the business model, the silver fleet sinks within sight of the port. The scientists are in sackcloth and ashes. What about the corona research, and it went so well?
You would say: Nobody gets Covid anymore, right? Hooray, actually!! But no: the scientists are at a loss and hint at higher doses of recent variants on older test subjects in order to be able to continue to develop vaccines against this life-threatening virus!
Transmission route
Of course, I was also curious about how exactly these infections are realized in that lab setting, always a source of hilarity.
We have in Playing poker with infections Already seen how difficult that is with respiratory viruses. Could it be that they put their test subjects on an exercise bike in an unventilated room with an atomizer that continuously generated infectious aerosols? Not at all.
What do we read in the reference study about the standardized method of inoculation:
Participants were inoculated intranasally by pipette containing 10 TCID50 of wild-type SARS-CoV-2 (100 μl per naris) distributed over both nostrils [...] and remained in the supine position for 10 minutes [...], followed by 20 minutes in the sitting position with a nasal clip on after inoculation to ensure maximum contact time with the nasal and pharyngeal mucosa.
A pipette! So with drops... And to prevent the droplets from being lost when inhaling and exhaling, they were given a nose clip for twenty minutes.
The study also states that lab workers were required to wear face masks. That's protection against splashes, but they probably think it also helps against aerosols. If you work with a pipette at BSL-2 level, you even have to work in a negative pressure box with extraction. After all, when dripping with a pipette, aerosols can be released...! ("aerosol-generating procedures" is what it's officially called). Imagine, that's dangerous, before you know it you're infected and infect someone else.
Protecting themselves against aerosols and trying to infect test subjects through droplets. Who gets it?
Somehow the awareness seems to be there, something with instinctive fears perhaps.
Epilogue: The Pandemic Treaty
Let me now turn to the pandemic treaty: centralised control by the WHO in the event of pandemics.
This study shows once again that you can at least fool doctors and medical scientists, perhaps the majority of all scientists, into believing anything. And it will stay that way, presumably until this entire medical generation is replaced. Not that everything is OK then, because the next generation will undoubtedly ride new hobbyhorses of their own.
They live on protocols. As soon as they get it from above, the thinking stops. Or vice versa: because they can't think, protocols have to be devised for them. Is contamination dose-dependent? OK, then we're going to increase the dose in the immunized. Is it via drops? OK, so a pipette. They don't really understand one iota of it, so if they strictly stick to the rules, at least they won't do anything wrong. See also our own OMT.
This is the generation of scientists that the WHO advises. What will they advise in the event of the next flu wave (including corona, of course, as has been the case for decades)?
a) Heavier vaccination. The doses we are working with now have become too low, you can see that from the fact that they no longer work well. The active dose of mRNA will have to be at least 100,000 to 1,000,000 times higher to generate any effect. This can also be achieved with more frequent vaccinations.
b) Stop vaccinating – after all, testing can no longer take place without CHIMS, so vaccination is irresponsible. That means strict enforcement of mouth masks, hand sprays, plexiglass partitions during the day, one and a half meters and after 6 p.m. -unfortunately it cannot be otherwise without vaccines- the curfew. And lockdowns if there have been spikes.
And then draconian imposed worldwide. In the Netherlands, we get it passed on through the EU, which sees something in centralized power. And all national government officials are bowing like flicking knives, half an eye on the European plush.
"Don't exaggerate, it's just a flu now?" Well, it was at the beginning of 2020 too...
The establishment lives in a parallel universe.
Also read the Follow-up post with more information about the vaccination statuses.
"They live on protocols" but thinking about money doesn't stop with most of them, I'm afraid. See also the reports on healthcare fraud. At the moment I let a number of friendships from that sector fade away, I am going to accuse them more and more in my mind of "death by guilt".
Anton, Jonathan Engler has also published about this:
https://sanityunleashed.substack.com/p/another-virus-challenge-trial-spectacularly
He extracts from table 2 in the appendix that of the 9 unvaccinated participants, only 1 contracts a 'community infection. That is indeed in that table that shows exactly how many injections the participants who contracted a community infection had.
So 13 out of 27 versus 1 out of 9.....
Take a look to see if it's correct. I think so.
What we mainly see is that people have no idea how infections work.
True! I couldn't find that Appendix / looked over it. I'm going to dedicate a separate article to that. Thanks Cees!
Especially the interpretation of LCMS of 28/02/20 is staggering. At the time, the analysis was 'good' ..... How is it possible that the matter has gone so off the rails after this very beginning of the plandemic? Something for further investigation (Anton, perhaps the parliamentary committee)? Furthermore, this is a great piece about how people are muddling along with COVID at the moment.
But something else is emerging on the horizon... What do we actually know about the next plandemic, H5N1? Isn't this also something for early research and alertness?
Fantastic.
There you are with your good behavior,
@MarionKoopmans
.
Your American friends are of the opinion that H5N1 – the bird flu virus – is not a Pathogen with Pandemic Potential. And that also applies, mutatis mutandis, to H7N5. We know that again.
According to them, we have nothing to fear from that.
Well, then we can abolish Viroscience. Glad to do so.
"However, human-to-human transmission has been rare and non-sustained. There are several MCMs or candidate MCMs that might also help to limit transmission depending on specific circumstances. Because A(H5) and A(H7) viruses do not transmit efficiently in humans, they are not considered PPPs in their wild-type state."
https://x.com/john_bumblebee/status/1787899024013508698
Good piece Anton. Any idea also how 'they'. have identified the asymptomatic route of infection? How? The only way would be to put people without C in a room with someone with C who doesn't sneeze, sneeze or cough, but talks. And then see which people are going to test POS on. This has never been investigated.
The only thing there was to determine whether someone had Covid or 'just' flu was a pos PCR test of which the CT values determine whether you find something. Above a certain CT value, you will always find something. It's a shame that our government refuses to release this data. It's all quackery in an expensive guise.