
The latest report from UKSHA, the official Health Safety Institute of the United Kingdom, is causing quite a stir. The data have been known for FOUR MONTHS and published a few days ago. Why something like this can take four months if you still watch over health safety, that is beyond my comprehension. An alert science journalist should have been able to deliver this news as early as November.
These dates don't come out of the blue. Before they were presented on 25 October 2022, they have already signed off before. It contains tables for July 2022. In May 2022 (two months before that) the JVCI knew nothing about it:
"Het herhalingsvaccinatieprogramma van vorig jaar bood een uitstekende bescherming tegen ernstige Covid-19, ook tegen de Omikron-variant."
Professor Wei Shen Lim, the chair for Covid-19 vaccination at the JCVI. (source)
waarmee hij terloops Omikron onder de "ernstige Covid-19" veroorzakende virussen schaart. Zoals we weten bestaat het Covid-19 syndroom niet meer en zijn de typerende symptomen bij Omikron van heel andere aard.
The dates were only presented to the members of the JCVI, het Joint Committee on Vaccination and Immunisation. Het werd geen groot nieuws. Bleef het in een academische Britse bubbel van "I got your back, you got mine"?
At least not British; One of the JVCI members is Prof. M.J. (Maarten) Postma, Professor of Global Health Economics UMCG & University of Groningen (Medical and Economics & Business faculties). I don't know if he was at the presentation. I can assume that he has been sent a PowerPoint or a handout. I couldn't do it myself minutes vinden en door de oudere notulen bladerend geven uitspraken als "Timeliness is more important than the type of vaccine" al een indruk van hoe de vlag er daar bij hangt.
Perhaps Professor Postma could give us a lecture on why you don't have to ring a bell for months when you have information that is vital to public health. It is always difficult to feel how hotemetoten think - excusez le mot.
Maurice de Hond posted yesterday in this article in which he showed a striking table from that presentation.
It concerns the number of vaccinations that must be made to prevent one hospitalization in low-risk groups. That number rises to 210,400. That sounds like a lot.

NNV (also: NNTV) is often used as a number of vaccinations needed to make a prevent infection but these are hospitalizations. Those numbers are higher.
John Campbell is also amazed when he goes through the numbers. Now I am not so introduced to NNV and hospital admissions so I try to get some feeling for the figures by calculating them to Dutch figures and in particular calculated by mortality.
An impression from The Lancet about NNVs against hospital admission
To get a sense of how high an NNV of 43,600 actually is, a few pieces and a graph from a study in The Lancet, over de NNV tegen "cases" van Covid-vaccins in de Pfizer-trials:
"...een daling met een vierde van de NNV (van 84 naar 64)."
"...een NNV van 217 (wanneer de ARR 0-84% bedroeg en de NNV 119 in de fase 3-studie)."
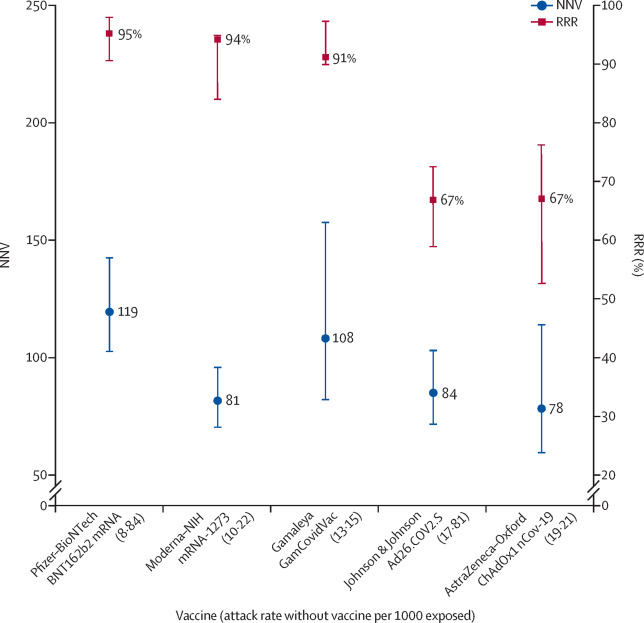
Look at the blue values, these are the NNV values. So this concerns dozens, up to the low hundreds. Actually, we're already done...
The Dutch situation
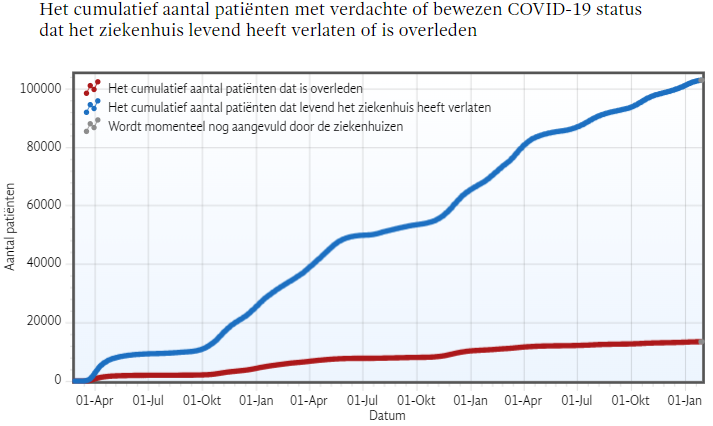
In the second half of 2022, the period in which children from the age of 12 were also allowed to be vaccinated in the Netherlands, we had 15,426 admissions.
Table 3C (above) runs roughly from 40,000 to 210,000. If you assume an NNV of 100,000, 1,542,600,000 (over one and a half billion) injections would have been needed to keep such a number of people out of the hospital.
If you think of the 80,000 prevented admissions (RIVM model...) you arrive at almost 8 billion injections.

Nu was Kuipers goed op weg naar die 8 miljard maar dat is hem toch niet gelukt. Zonder dollen: dit zal methodologisch vast wel aanvechtbaar zijn. Zo zijn vaccins effectiever geweest bij een "naïeve" populatie maar er lijkt desondanks wel iets aan de hand met de ordegroottes.
According to Statistics Netherlands, 2,500 Dutch people with and because of Corona died in those 6 months. That's 17% of those 15,426 hospitalizations. Of course, those who died also include people who gave the ghost outside the hospital. Apparently, there are often circumstances that lead to no longer going to the hospital with Covid symptoms such as increasing respiratory distress, etc. If that's because they're all 90-year-olds, that should lead to a completely different kind of rethinking, but we'll take that fact into account as well. It is plausible that this 17% keeps pace with hospital admissions.
Hoe de codering bij CBS precies verloopt, op basis van WHO-instructies, is niet transparant. Iemand zou kunnen denken dat "Covid-19" wordt aangevinkt als ergens op het B-formulier corona of covid wordt genoemd. In het begin van de coronacrisis waren de CBS-cijfers twee keer zo hoog als die van rivm, inmiddels is het VIJF keer zoveel covidsterfte volgens het CBS. Hoe dat zo veranderd kan zijn is niet helemaal helder.
Voor het "alleen door corona"-scenario houden we stichting NICE aan. Over die periode is het covid sterftepercentage daar ruim 7% van de covid-opnames. Maar er is een duidelijke dalend trend: Januari 2023 komt op ruim 6%. Besturen is vooruitzien dus met het oog op de toekomst nemen we 6%. We laten twee tabellen zien om de range aan te geven, de ordegrootte waarbinnen gedacht moet worden bij deze controversiële mRNA-vaccinaties:
- With Corona
100/17 = 6, rounded. This means that we must multiply the NNV by six to prevent one death, if we use CBS figures ('with' corona). That's Table A. - By Corona (based on NICE figures)
100/6.3 = 16. This means that we must multiply net NNV by 16 to prevent one admission to prevent one death if we use 'plausible' figures ('due to' corona, explanation in the box). That's Table B.
If anyone wants to take the trouble to work through these calculations per age group, please! I'm keeping the ballpark figures now. That yields the following two tables, choose the most likely one yourself and think about what that could differ per age group.
NNTV NL - Number of vaccinations required to prevent 1 death in the Netherlands
| Basis: CBS figures Total corona mortality as 17% of hospital admissions | |||
| Low-risk group | Basic series | Booster (2+1) | Fall booster '22 |
| 20-29 | 119.400 | 203.400 | 1.009.200 |
| 30-39 | 130.200 | 322.800 | 1.262.400 |
| 40-49 | 130.200 | 269.400 | 555.000 |
| 50-59 | 65.400 | 94.800 | 261.600 |
| Basis: NICE figures Totale "door corona"sterfte: 6% of hospital admissions | |||
| Low-risk group | Basic series | Booster (2+1) | Fall booster '22 |
| 20-29 | 338.300 | 576.300 | 2.859.400 |
| 30-39 | 368.900 | 914.600 | 3.576.800 |
| 40-49 | 368.900 | 763.300 | 1.572.500 |
| 50-59 | 185.300 | 268.600 | 741.200 |
This is based on the premise that you can estimate the total mortality by taking 6% of all hospitalizations.
If you assume half, you must double the NNTV - and vice versa.
6% chance of death from corona hospital admissions: this percentage is calculated on the basis of NICE Foundation. (January 2023 from Chart 1)
We then assume that the typical covid patient goes to the hospital. Reasons for not doing so may include other diseases or high vulnerability, often accompanied by old age. The question is then justified whether these people die a natural death or die too early from covid. A positive PCR test without fatal covid disease is also conceivable.
Lack of data on side effects leads to polls and research
Trials
Noch de originele Pfizer-papers, noch de contra-analyses, noch obervationele data tonen aan dat vaccinatiesterfte onder deze grenzen blijft. Dat is immers wat wordt bedoeld met de vage kreet "The benefits outweigh the risks": er mogen best mensen doodgemaakt worden, als het er maar net iets minder zijn dan degenen die de farmaceut effectief heeft beschermd. Dat is iets anders dan "First do no harm". Alleen body bags worden geteld en van elkaar afgetrokken - hoop je dan, want ook dat gebeurt niet openlijk. Over vaccinatiestatussen wordt schimmig gedaan. Er wordt bij die benefits/risks rekensom ook niet naar verloren levensjaren gekeken, wat de balans zou doen omslaan. Dit om nogmaals aan te geven dat de hele ketting per leeftijdscategorie goed moet worden bekeken.
Polls: Steve Kirsch finds confirmation in published paper
Papers and studies with frightening numbers are regularly published, for example these: The role of social circle COVID-19 disease and vaccination experiences in COVID-19 vaccination decisions: an online survey of the U.S. population, which calculates that, based on a survey of 2,840 people in December 2021, 215,000 to 335,000 Americans died from Covid shots in 2021 alone. The (in our view somewhat dubious) research comes from economist Mark Skidmore, who has a chair at Michigan State University. The clever twist he makes is that people at least HAVE THE IMPRESSION that there are hundreds of thousands of vaccine deaths. That is not good for vaccination willingness - and that is of course important!
The structure of this published paper is reminiscent of the polls of Steve Kirsch who feels quite confirmed because the results confirm each other. I am less enthusiastic about the harshness of this methodology. It is clear that this type of research leads to this kind of results.
How it should be done: representative research
Coincidentally, Maurice also posts today an article with a study on covid/vaccination perception. Steve Kirsch's polls were always criticized for the respondents coming from their own bubble. At Maurice we are talking about a REPRESENTATIVE sample, that is different cake.
With NNVs running into the millions, you really have to scratch your head. It would undoubtedly have been less bad, but the fact that something like this could continue is harrowing.
First the dates on the table, at least in the Netherlands!

Are you looking at: https://www.maurice.nl/2023/01/29/wat-denkt-nl-over-de-oorzaken-van-oversterfte/
If you ask the citizens, who voted CDA-D66-Grlinks-VVD and PvdA, almost all think that the excess mortality can NOT be due to the vaccine.
Look in my surroundings, it's actually exactly the same. Vaccine is not partly / possibly the cause. So citizens with this opinion, are in the majority, how are you going to convince them??
I can't do it, in my own family, with these thoughts.
Doctrine and influencing citizens, government has worked well. 🙁