
There are two routes through which a disease can end up in Group A. Hugo de Jonge writes in response to a parliamentary question that "the classification of an infectious disease in group A, in the Public Health Act (hereinafter: Wpg) is related to the question of whether national control is considered necessary by the Minister of Health, Welfare and Sport (hereinafter: VWS). If that is the case, then the disease is classified in group A."
This is an incomplete description. First of all, it is good to know that the Council of Ministers can legally place an infection temporarily on the A-List, if "the feeling of the Council of Ministers" that indicates. For example, if the Council of Ministers sees a great danger to public health, expects to have to implement drastic measures in the very short term, wants to encourage the use of a digital pass or is simply in complete panic (my free translation of the term "feeling of the Council of Ministers"). Legally, no doctor needs to be involved here.
However, this route can only be followed under the following legal conditions:
- a cause of the disease unknown according to the state of science
- a well-founded suspicion of contagiousness
- serious danger to public health
At a glance, including that of a member of parliament, it can be seen that Omicron now only scores on point 2. Omicron is contagious – but so are colds and herpes. There are viruses for which the entire population tests positive (there are 140,000 viruses in our intestines alone).
The 'feeling of the Council of Ministers' can now really no longer be that all measures, including the QR pass, are permissible because of the disease. Maybe there is another reason but it is not communicated. You don't hear the Council of Ministers about it, they leave it to the medical advisors. This disproportionality has caused trust in the government to sink to an all-time low.
Also pay attention to the use of "related". In doing so, de Jonge deliberately leaves open whether it is cause or effect. You would almost think that it is a sufficient argument to say: "national control is desirable", while that should be the policy response to the observation that we are dealing with a serious disease.
The experts have never tested Omicron against the above three legal points, of which only point 3 is important. The experts do not go through the decision tree (see below) either. The Senate has not looked at these conditions either. Everyone is satisfied with the instinctive "feeling of the Council of Ministers" at the time, in early 2020: go ahead with list A. So no distinction has ever been made between the situation with the 'new, unknown' virus at the time and Omicron, about which we now know much more than what was known about the Wuhan variant at the time. (see the bullets in the previous post)
(Re)evaluation of a disease
1) Don't just follow procedures
In order to make such a temporary situation proportionate again as soon as the initial panic has passed, the law provides for later mandatory extension procedures. The intention is that testing will then take place.
These tests do not appear to be functional for determining severity. Neither the virologists involved, nor the ministers (the kongsi OMT/cabinet) will be eager to give up the newly acquired attention and power, so the signals do not jump green quickly. Moreover, they are born risk averse, so it is easy to point out enormous potential dangers with every speck of risk.
Who should then test whether that risk is still real? The doctor can say so much... Where is the second opinion?
Not much can be expected from the House of Representatives, which votes with the cabinet. After that, the Senate is mainly a procedural formality: "Is it all possible?" and not: "What are we actually doing?". (I always thought that, that there was also some reflection.) But the disease itself is simply no longer tested and so undemocratic arrangements can be maintained until the end of days. They can be enshrined in emergency laws, in the health law – as long as the medical profession does not get in the way. But why should they.
It was also evident from Ernst Kuipers' justification in the Senate: he pointed to the past, how bad it had been, that virus from 2019. No one said: 'It's 2022 now, you act like we have the same flu every year'.
What was especially important in his argument: the uncertain future, how bad it could get. But he could have told that story in 2018 or in 2019. Just like that. Or because we had just finished the horrible flu epidemic '17-'18, with no less than 9,500 deaths in 1 year, considerably more than in the average SARS-CoV-2 year.
No one in the Senate said: 'It's 2022 now, you act as if we have the same flu every year'.
Would we have wanted to live under a technocratic regime in 2018 and 2019 and surrender our fundamental rights, just because a group of 'experts' had warned that after 2017-2018 there could be another terrible new influenza wave? Worse than ever? (And then you will just see: then in 2020 it turns out not to be influenza but something else...)
2) The decision tree: when the dust has settled a bit
Unfortunately, what Kuipers did not do was point to the current Omicron situation in February 2022: a virus that approaches the innocence of a cold.
"It can go either way," Kuipers threatens and he misinformed the Senate with disinformation about a mortality rate of 0.9%. Our virologists do not put this into perspective by informing this MDL doctor. The mortality rate is currently between 0.003 and 0.03 (source: Herman Steigstra).
A virus usually mutates into increasingly mild and contagious forms (as I just encountered again in this Nature article). If OMT doctors were to confirm that good news, they would immediately lose their privileged position because then it would be clear that there is little left to fear from the current "SARS-CoV-2" – at least not the Covid-19 disease.
"Omicron-21" could be a correct name for the current clinical picture. Or "Omicron" for short, just like the virus. After all, the disease SARS is also called the same as the virus. While with Ebola it is the other way around, which can be caused by as many as five different Ebola viruses, a virus group named after the disease it causes. In any case, Omicron is not a "Covid-19".
An independent OMT would want to test a mutating epidemic virus every quarter against the legal powers, but that is not in their interest now. While it is in the spirit of the law; After all, that's why those extensions were invented. That is to look at again and again: are we going to extend or not and why, what is the situation now? There is a decision tree for that, see below.
As long as you close your eyes to the differences between diseases, you can keep filling your toolbox. Hop, another 30 million for an app update. Why on earth!? What exactly did that app contribute, Dancing with Jansen? Now I've also made an app and I have to say, this seems pretty hefty to me – but then again, I'm not a virologist.
Group A, B1, B2, C: groups of diseases with a notifiable obligation and their own measure ceiling
Experts should advise on the severity of a disease on the basis of the decision tree below, according to the RIVM. For those who have read the previous Open Letter, it will be clear that there is no route for Omicron to the "Advise reporting obligation" box, other than perhaps via the International Health Regulations which only says something about the obligation to report so that it is signaled when a disease rears its head somewhere and monitoring of the reports.
Nothing about an A-status, only Covid-19-specific Temporary Recommendations such as "work risk-based" (so no universal mandates and obligations) and "do not use vaccinations as an obligation for international travel" (which discourages a 2G application for the QR pass).
Below is the decision tree of the experts. Walk through it with Omicron in mind. Start at Start. You will not receive two hundred euros.
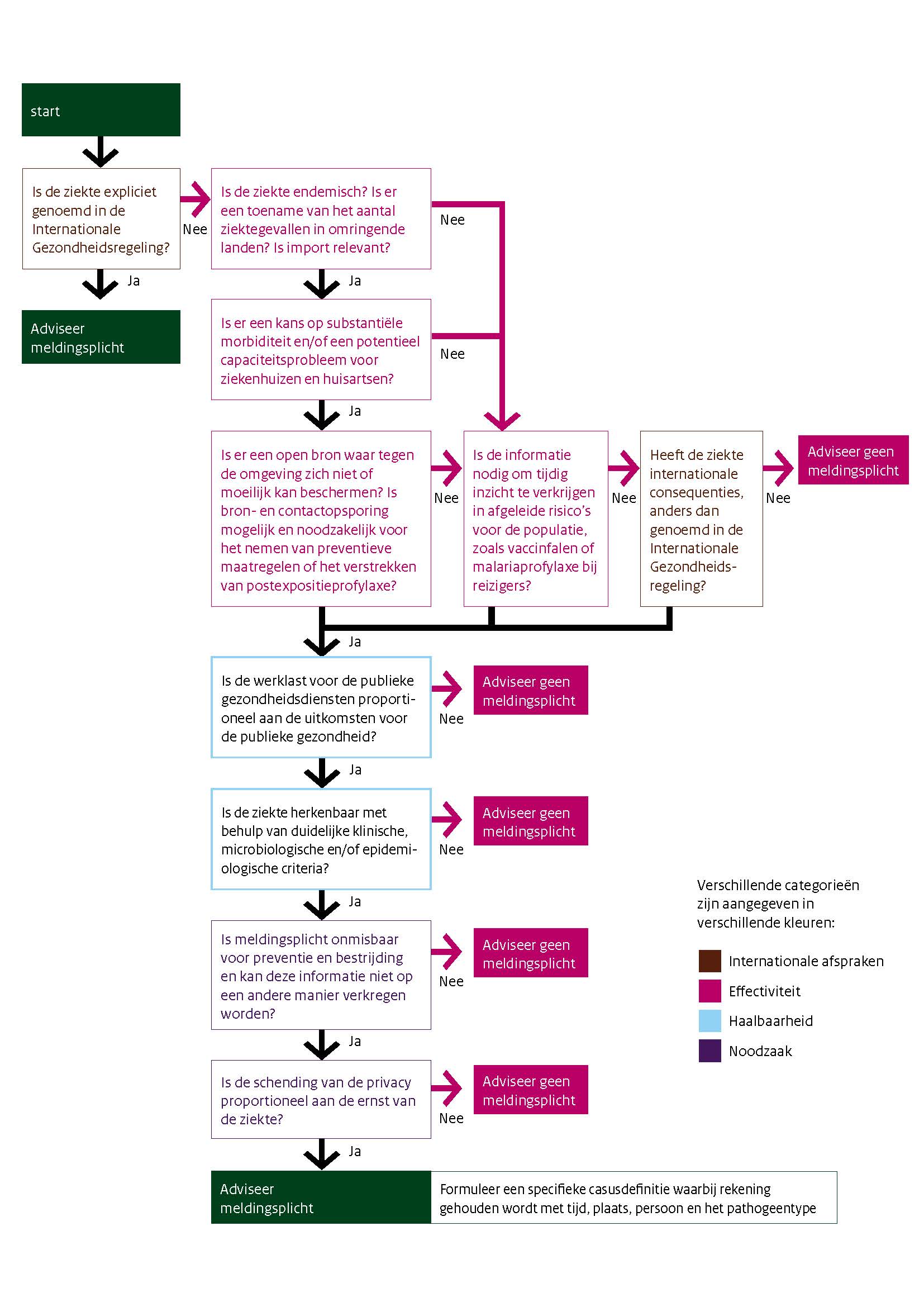
To pick a few: there is no increase in the number of cases in surrounding countries, imports are irrelevant. Endemic? Kuipers said yesterday that he did not, but that doesn't say much, after all, he is not a virologist and works with bizarre percentages that are manipulated graphs to rival.
There is also no chance of substantial morbidity. And so on; Not a chance. Of the bottom four decision points, none leads to "Advise on the obligation to report". Omicron is really a soft egg among pandemics.
But then again, this is apparently no longer tested. That too is an explainable habit: after all, we have never had such a rapidly changing disease on the A-List before. That makes no sense at all: the point of the list is that you immediately know what to do when a certain disease (re)appears. But a virus whose disease changes character almost every six months is no longer a shadow of what it was in 2019, when it came fresh from the lab – or from that one pangolin, of course. So what should you put on that list now? The Spanish flu? That calls for a draft motion.
Covid-19 has been declared a pandemic in the International Health Regulations, that would make the obligation to report unavoidable. After all, that means that we are dealing with a worrisome disease. The experts then advise on which Group the disease must be placed. A suitable package of measures has been devised for each Group. But as argued: we no longer have Covid-19 and the Omicron disease has still not been declared a pandemic after more than two months.
The government does not distinguish between viruses that hardly mutate and viruses that can change within a month in such a way that they cause a completely different clinical picture (such as from lungs to throat). Doctors should be on top of that, it is essential.
Oh dear, the future...!
Referring to a possible future catastrophe is a recurring figure of speech that actually suits the incumbent a little too well. They are never judged on it because the catastrophe invariably turns out to be averted, of course by decisive intervention. However, never before has so much misery been caused on the basis of such an uncertain threat, in ways that go against the principles of a democratic constitutional state. And that is exactly why a new law is needed: to be able to legally violate fundamental rights.
Now we each house hundreds of thousands of viruses in our bodies (with bacteria together accounting for one and a half kilos), but has that ever been a reason for a toolbox with fundamental rights restrictions? By the way, don't tell Kuipers, who will have a heart attack when he realizes what can happen if even one of all those microorganisms were to mutate malignantly.
Toolbox or App drawer?
What good are all fundamental rights-restricting tools: face masks, of which it has been clear for a long time that they do not stop a pandemic. That can't be it. Lockdowns, which at most spread the number of deaths over a longer period of time at massive public health loss and cost... It can't be.
So why the drive to keep fundamental rights restrictions in the toolbox? The curfew that the incoming Minister of Health, Welfare and Sport determined did not work at all? Is it the flattering positions of advisers and the unbridled room for manoeuvre of the minister? To be important, to join talk shows? Or the preparation for a more technocratically directed society?
So then we have arrived at the CTB, the stepping stone to the EU pass, but would the cabinet really want to be the most well-behaved child in the EU/WEF class? At the expense of freedom and democracy? Has the Netherlands been put forward as a pilot country, the ideal digital testing ground on top of Europe's most important internet exchange? After all, we have the best infrastructure! And you know, technology is unstoppable anyway. And how else are you supposed to distinguish yourself, as a cool little country...
Motion Theunissen on Spanish Flu in group A
The Chamber,
after hearing the debate; whereas Covid-19 has been included in Group A in order to be able to immediately resort to unconstitutional measures in the event of a predetermined coronavirus outbreak, unhindered by parliamentary intervention or other delaying formalities;
Whereas, that this essential protection of public health is lacking in the event of suspicions of other virus outbreaks;
noting, that it is currently not possible to intervene quickly in the event that a vaccine or virus expert foresees an influenza virus outbreak;
calls on the Government to place the Spanish Flu in Group A in order to close this gap;
and expresses as her wish, that in the event of possible imminent flu outbreaks, unconstitutional measures can and will be taken immediately to offer the people the legally prescribed protection.
and proceeds to the order of the day.
Relevant attachments are listed under the previous post