
There are still people who deny the excess mortality in 2021 or who simply want to follow the CBS story that it is all Corona-related and that there were only certain moments of slight excess mortality. For these people, vaccine mortality should not be a subject of research. The studies calling for 'raw data' are piling up, precisely to rule out vaccination. All statistical analyzes show an obvious correlation; so strong that causality is sometimes difficult to escape.
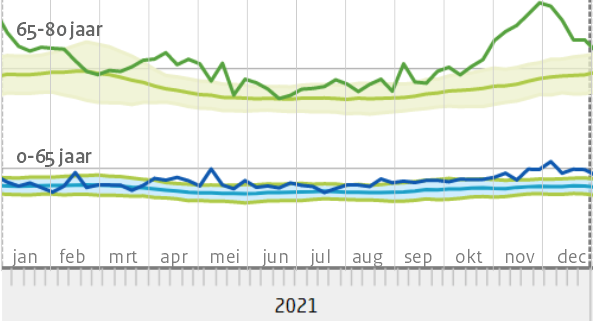
The most obvious is the excess mortality in the group of 65-80 years. But we also noticed a relatively large excess mortality in younger groups at an early stage. In a group in which there should be no to very little excess mortality, it is soon relatively large. Not only in the Netherlands are the data that could shed light on this, carefully protected by governments. Nevertheless, the picture is becoming more and more complete, also through analyses from abroad.
A number of puzzle pieces come together in pierre Lecot's article from last week (March 27), in France Soir. A thorough article in which he statistically substantiates the European and French excess mortality, also pointing to four analyses from other countries. Below are a total of five very short (and therefore certainly incomplete) summaries of these articles, with the emphasis on the 50-somethings.
Pierre Lecot in France Soir: EU, FR and other countries
https://www.francesoir.fr/opinions-tribune/surmortalite-en-europe-chez-les-jeunes-depuis-cet-ete
In een long-read in France Soir behandelt Lecot de leeftijdsgroep 15-44 jaar. Eerste belangrijke constatering (die de virusvaria-lezer bekend zal voorkomen) is dat ook als de "oversterfte"-lijn niet wordt overschreden, de sterfte toch abnormaal hoog kan zijn. Voor meer statistische uitleg dat we het wat dit betreft bij het juiste eind hadden, zie het originele artikel.
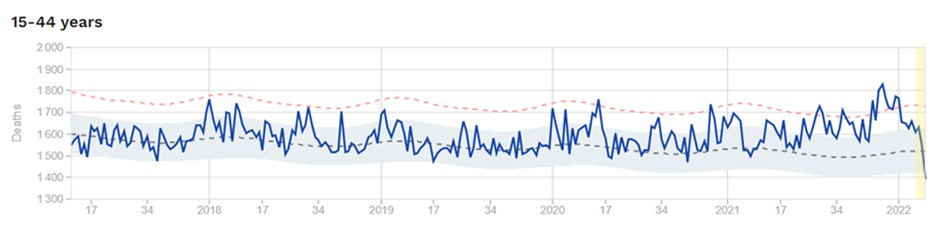
He then makes various comparison models in which he traces mortality trends. Seasonal mortality (which differs per age group: young people die more often in the summer because of risky behaviour) and population pyramids are taken into account. Whatever method he uses in his analysis does not matter: excess mortality is undeniable, even in the younger age groups. The red bars show excess mortality in Europe, here those of the age group 15-24 years (!):

In Frankrijk is de Senaatscommissie gevraagd om dit fenomeen te onderzoeken. Dat verzoek is zonder opgaaf van redenen geweigerd. De vragen die daarbij worden gesteld: "Waar kan de Eerste Kamer bang voor zijn? Waarom zou de analyse van de mortaliteit na injecties van veilige en effectieve vaccins problematisch zijn? Hadden we de sterftecijfers na de injecties niet meer dan een jaar moeten volgen? Vooral voordat je ze aan kinderen aanbiedt en opdringt of verplicht aan iedereen ouder dan 12 jaar?"
He then runs the same analysis on other European countries and compares the timing of the red bars with the vaccination periods. Several striking graphs are in the article. He comes to the conclusion:
"De sterftepieken liggen te vaak dicht bij vaccinpieken om het aan toeval te wijten te zijn."
From: https://www.francesoir.fr/opinions-tribune/surmortalite-en-europe-chez-les-jeunes-depuis-cet-ete
Germany: comparison of Bundesländer (a.l.)
The results (across all ages, including young people) show that both the mortality course in 2021 and the course of excess mortality with some delay reflect almost exactly the course of the first, second and booster vaccination: If the number of vaccinations increases, the number of deaths or excess mortality increases, if the number of vaccinations decreases, the number of deaths or excess mortality decreases shortly thereafter. Some points that emerge from the empirical picture:
- The correlation is very strong: this is shown, for example, by a daily correlation analysis (7-day moving averages) of the German data. For example, the course of excess mortality (increase in mortality in 2021 compared to the average of the previous five years) in the period from the beginning of March to the end of May correlates with the first vaccinations at a level of r = 0.95. The connection pattern is currently being analyzed using more complex statistical methods, and the first results confirm the strong connections
- The link is observed despite different vaccination patterns: an analysis at the level of the individual Länder shows that excess mortality varies according to the state, depending on the specific vaccination pattern of a state.
- Such a correlation can be seen in all other countries that have been examined in more detail so far. A cross-country analysis of 15 countries with available data on booster vaccination and excessive mortality shows a very high cross-country statistical relationship between excessive mortality and vaccinations.
- Uitsluiting van mogelijke verklaringen van "confounders" (een derde variabele): Een analyse van mogelijke derde variabelen toont aan dat voor de hand liggende derde variabelen zoals het aantal COVID-sterfgevallen of het aantal SARS-CoV-2-infecties het waargenomen verband tussen oversterfte en vaccinaties niet kunnen verklaren.
The observed pattern of findings suggests a causal effect according to the usual criteria for inferring causal conclusions from observed correlations in medical research.
So much for the highlights from Germany.
The number of COVID deaths or the number of SARS-CoV-2 infections cannot explain the observed link between excess mortality and vaccinations.
From: https://osf.io/5gu8a/
Young adult mortality in Israel during the COVID-19 crisis
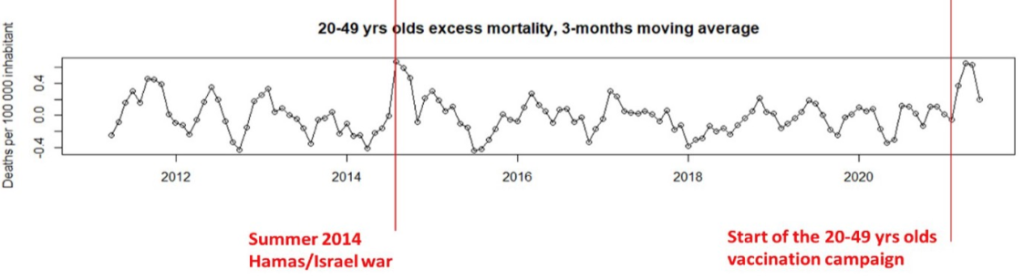
Young adults under the age of 50 have a low susceptibility to COVID-19 mortality. Dataof the Central Bureau of Statisticsof Israel show unexpected rise in excess mortality among 20- to 49-year-olds in February-March 2021.
Excess mortality peaks among these young age groups are rarely observed. If it occurs at all, it is with a low number of deaths caused by wars, for example. The increase in mortality in 2021 coincided with the rollout of the Israeli vaccination campaign for the 20 to 49-year-olds. Because similar increases are also observed in other countries, that is reason to pause the campaign and at the same time clarify the underlying reasons for those additional deaths, especially in the context of a low mortality risk from COVID-19 in adults under the age of 50.
There is an inconsistency between the official COVID-19 deaths and additional deaths under the age of 50 as of February 2021. To rule out that that could be because of the vaccinations [apparently they too do not have the necessary raw data], the researchers look at differences between countries with 'mass vaccination' and with 'moderate vaccination' (among the younger age groups).
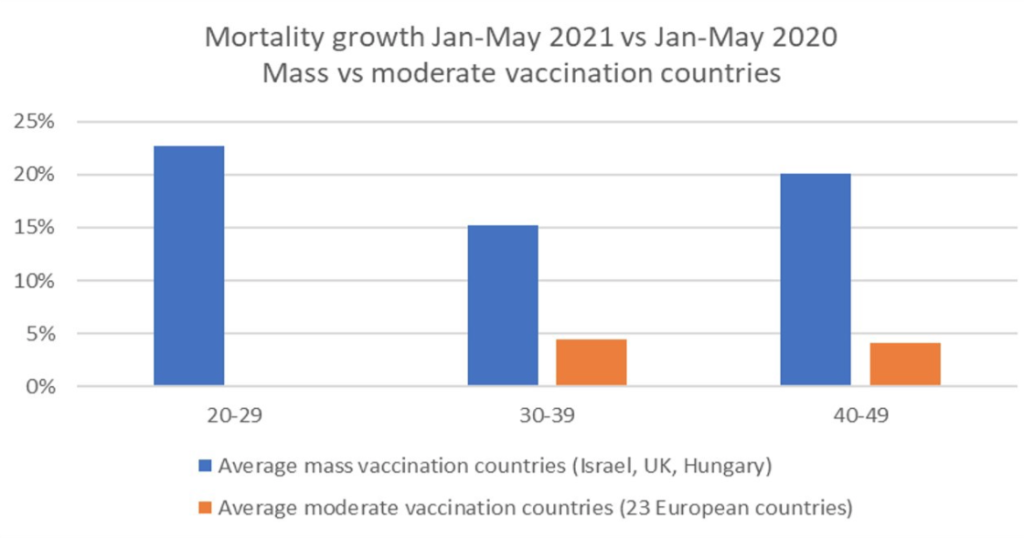
The mortality peak among 20 to 49 year olds in February-March 2021 is therefore unprecedented and even worrying. The researchers refer to a study by Retsef Levi that documents a 20 to 35% increase in cardiac arrests among Israelis aged 16-49.
They also decide with
"Een dergelijke opeenstapeling van bezorgdheid zou naar onze mening dringend moeten leiden tot een pauze in de vaccinatiecampagne, totdat de redenen van de oversterfte onder jongeren in massavaccinatielanden zijn opgehelderd."
From: https://steve-ohana.medium.com/young-adult-mortality-in-israel-during-the-covid-19-crisis-ff7456cff74f
United States: COVID vaccination and age-stratified mortality
[translation of the 'Abstract']
In this study, regional variation in vaccination rates was used to predict all-cause mortality and non-COVID mortality in subsequent time periods using two independent, publicly available datasets from the U.S. and Europe (monthly and weekly-level resolutions, respectively).
Vaccination correlated negatively with mortality 6-20 weeks after injection, while mortality was predicted in the 0-5 weeks after injection. This in almost all age groups and with an age-related temporal pattern that is consistent with the administration of vaccines in the U.S. by age group.
Results of adjusted regression slopes (p<0.05 FDR-adjusted) suggest a nationwide mean VFR [Vaccine Lethality Ratio] in the U.S. of 0.04% and higher VFR with age (VFR=0.004% in ages 0-17, increasing to 0.06% in ages >75 years). This means 146,000 to 187,000 vaccine-related deaths in the U.S. between February and August 2021.
Vaccination in adults notably increased mortality among unvaccinated young people (<18, USA; <15, Europe). [I don't see an explanation for this] Comparing our estimate to the CDC-reported VFR (0.002%), it suggests that VAERS deaths are underreported by a factor of 20, consistent with the well-known VAERS bias for underestimation.
Comparing our age-stratified VFRs to published age-stratified mortality rates for coronavirus infections (IFR) suggests that the risks of COVID vaccines and boosters outweigh the benefits in children, young adults, and older adults with low occupational risk or previous exposure to coronavirus.
We further discuss the implications for public health policy regarding boosters, school and workplace mandates, and the urgent need to identify, develop and disseminate diagnostics and treatments for life-changing vaccine injuries.
The benefits of COVID vaccines and boosters do not outweigh the disadvantages in children, young adults and older adults with low occupational risk or previous exposure to the coronavirus
From: https://www.researchgate.net/publication/355581860_COVID_vaccination_and_age-stratified_all-cause_mortality_risk
[In short: only among the vulnerable do the advantages outweigh the disadvantages. This means that there are slightly fewer deaths from the vaccine than from the disease. Ethical issue: A vaccine that kills 99 random people and prevents the 'natural' virus death in 100 others, do those advantages outweigh the disadvantages? And at 75? At 50...? etc. There was a time when a handful of suspected deaths was already a reason to stop vaccination campaigns. ]
Machine Learning analysis of US and EU data
This is a statistically very interesting article that mainly explains how to deal with uncertainties, bias, mismatches in databases, causality and other variables. Bayesian analysis comes along, bias-free machine learning and what kind of influence that can have, etc. While reading, you get the impression that sometimes you'd better just use your common sense!
Ze introduceren een "DoseRate" en een "CaseRate" en stellen die tegenover elkaar. Enfin, ze komen toch tot solide bevindingen.
"Voor de leeftijdsgroep van 04-44 jaar hebben vaccins duidelijk geen nettowinst op oversterfte. Het feit dat de vaccins aan een belangrijk deel van de bevolking zijn afgeleverd, betekent dat zelfs een kleine toxiciteit verantwoordelijk kan zijn voor evenveel sterfgevallen als de ziekte zelf."
and after a few more reflections:
"Desalniettemin ligt de oversterfte van 2021 in de EU ruim boven de oversterfte van 2020 die op zijn beurt weer ruim boven die van 2019 ligt. Het lijkt erop dat de variabele COVID-19-Death-Rate niet voldoende is om de stijging in 2021 te verklaren."
And:
Onze variabele DoseRate, gerelateerd aan COVID-19-vaccins, verklaart blijkbaar een groot deel van de sterfte die wordt waargenomen in de categorie 0-44 jaar."
From: USE_MORTALITY_IN_EU_IN_2021_A_MACHINE_LEARNING_PERSPECTIVE
In Australia, One Nation is done with it
One question: how on earth do you think you're going to get away with this? We won't let you get away with it; we're coming after you. We have the stamina to push you until you run out of steam - and we damn well will.
Malcolm Roberts, Senator for Queensland (Australia), in Parliament. Out of his speech to the Senate
