
This is my response to objections I received regarding my Ivermectin article of March 30, about the Africa effect.
Introduction: Begging for Randomized Controlled Trials
Why the producer of ivermectin does not pull the cart
An unsound investigation
A hopeful piece in The Lancet
The price of ivermectin
Is the European Medicines Agency also against it?
Side effects ivermectin
Search for other explanations for the correlation in the graph
"The expected low mortality rate would require an unfeasibly large sample size to provide sufficient strength for a study of effect on mortality."
The above quote is a regular feature in studies on combating Covid mortality. Actually, you might wonder why there is no way to investigate the risk of death in diseases with such low mortality rates. Mortality is so low that perhaps such importance has not been attached to it before? Who knows.
Too small studies, that's true
Most publications are small initiatives by doctors and scientists who describe their observations. They have the experience that a certain treatment has a positive effect and therefore insist on a large RCT (Randomized Controlled Trial).
Meta-studies take stock of all studies - including the ones mentioned above - and if they conclude that studies could not significantly show that the treatment works, they are not telling anything new or interesting. You may even wonder what the point of that conclusion is – or perhaps what the intention of the meta-study was. In any case, it is fodder for the media, which then see scientific proof that the treatment does not work. It is a way of thinking that can hold things up well in times of crisis.
Where are the large RCTs then?
There are few organizations that have the resources and especially feel the interests to invest in possible evidence that a cheap-to-produce patent-free drug, in this case ivermectin, can make Covid mortality even lower than it already is. In such an investigation, everything has to be right – which certainly does not always work. Sometimes incidents occur during such a tightly organized investigation that make things go wrong. It's quite a circus; an expensive affair.
There are also structural problems: for example, the research group has to run into tens of thousands if you want to have hard evidence for minute differences. The importance of pumping up small samples via statistical tests is also a proven technique. A positive effect is repeatable time and time again. Each repetition separately is not statistically significant. The methodology must also be correct and only one thing has to happen for your statistical ambition to evaporate before your eyes.
Statistically significant evidence of mortality reduction is a problem. After all, most people do not get sick anyway, and if they do get sick, they get better in most cases (99.85% of the total group). Until now, high-risk groups have been excluded from studies on ethical grounds, while it is precisely there that mortality has increased due to Covid. So there is very little measurement result left between the background noise of disease and mortality in each population.
Competitors of ivermectin have it easier: they only have to fund studies that, due to the design or size, will not be able to demonstrate that ivermectin has an effect. Especially when it comes to mortality, that's easy. An independent methodologist could assess this, even in advance. Unfortunately, journalists - and this also applies to many doctors - know little about methodology. The media will make it that ivermectin has been shown not to work after all. (Headline Volkskrant: "Acclaimed 'miracle drug' ivermectin does nothing against corona")
And what about the producer of Ivermectin?
Companies that could invest in it are pharmaceutical companies such as Merck, the current producer of ivermectin. However, Merck has publicly confirmed that it is advising against ivermectin as a Covid drug and has also stopped developing its own corona vaccine. A month later, it was announced that the contract negotiations had been completed and that they had signed for the co-production of the Janssen vaccine. More details in the replies below.
Be that as it may, most ivermectin studies do not come to significant results. As a result, it is easy to conclude that Ivermectin does not work. If you read those studies, you will come across other information.
I therefore derive, very unscientifically (I know), hope from a finding such as "While the result showed a significant benefit for ivermectin use in terms of an 85% reduction in mortality, it was admitted that the certainty of the evidence was very low." Where is that big, well-set up RCT!?
News-medical.net, February 1
Unfortunately, no one on LinkedIn has discussed the recent studies and graphs from other parts of the world with which the article concludes. Well-known studies and other objections are presented as proof that Ivermectin would not work. I will discuss them below, and then I will be done with this topic for the time being. By the way: the overall mortality in Africa is a lot lower than in Europe. This may have to do with the heat and humidity – although we will see in the last argument that these differences do not matter on the spot.
The rehearsals to the objections
Argument 1: Ivermectin is discouraged by the producer
The manufacturer has declared the drug itself unsuitable for use in Covid patients
If a producer sees the opportunity to become a co-producer of a vaccine to be rolled out worldwide every six months, it would be bad entrepreneurship to instead promote a pill whose patent has long since expired. Shareholders will ask questions. Janssen has also played excellently: they have scaled up their capacity and at the same time eliminated an important competitor. See the development below.
Merck discourages Ivermectin – timeline
- 25 January, 2021 6:45 am ET
KENILWORTH, N.J.–(BUSINESS WIRE)–Merck (NYSE: MRK), known as MSD outside of the United States and Canada, today announced that the company is discontinuing development of its SARS-CoV-2/COVID-19 vaccine candidates.
- February 4, 2021 11:45am ET
KENILWORTH, NJ – Merck (NYSE: MRK), known as MSD outside the United States and Canada, today reaffirmed its position regarding the use of ivermectin during the COVID-19 pandemic. We continue to carefully examine the findings of all available and emerging studies of ivermectin for the treatment of COVID-19 for evidence of efficacy and safety. It is important to note that our analysis to date has shown:- No scientific basis for a possible therapeutic effect against COVID-19 from preclinical studies;
- No meaningful evidence of clinical activity or clinical efficacy in patients with COVID-19 disease, and;
- A worrying lack of safety data in most studies.
[Still, a note: "A worrying lack of safety data" is reason for Merck to discourage a drug of which it has already sold billions of doses. I'm open to explanations.]
- 2 March 2021
MSD to help with the production of Janssen's 'Leiden vaccine'. Op 2 maart 2021 kondigden we onze samenwerking met Johnson & Johnson (het moederbedrijf van Janssen) aan, waarbij we in de VS productiecapaciteit ter beschikking stellen.
So not much can be expected from that corner.
Argument 2: Scientific evidence that Ivermectin does not work
https://jamanetwork.com/journals/jama/fullarticle/2777389
I had already discussed this research. It is a lousy study, destined not to yield any significant results. See my previous blog of 5 March. 10 days later, even more came to light: judging by the data, the control group also used ivermectin. That is for sale in Colombia. It is remarkable that they then fall through the cracks when they report their side effects as well... The differences are disappointing, of course. The article is also discussed in the interview by Vincent Everts with Pierre Kory of 19 March.
Argument 3: More scientific evidence that Ivermectin doesn't work
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(20)30464-8/fulltext
I get a lot of links to articles that I 'should read' because I don't know anything about them. To my surprise, those articles usually confirm my own point of view rather than that of the opponent, or they are articles that were the subject of my criticism and could undeniably be undermined. That doesn't help. This research surprised me again, because it is very positive about ivermectin!
"This pilot shows a decreasing tendency of the 'viral load' in the Ivermectin group, a decreasing tendency of the IgG titers that may reflect milder disease and clinical benefit in main symptoms of COVID-19 related to tissue damage: anosmia/hyposmia [loss of taste/smell] and cough.
These results are consistent with growing evidence from studies in Bangladesh [[10], [11]] and Argentina [[12]] showing faster viral clearance in treated participants, as well as recent data from a SARS-CoV-2 hamster model from Institute Pasteur that also showed a clear gender dichotomy in the effect of ivermectin on anosmia/hyposmia."
"All patients completed the 28-day follow-up period. There were 15 adverse events (7 in the ivermectin and 8 in the placebo group) that were experienced by 10 patients (5 in the ivermectin and 5 in the placebo group). There were no serious side effects."
It makes you think that apparently no more definite research could be found. Or that someone does not fully understand the matter or just forwards it to the left without looking at it critically. What was wrong with this article... Maybe they thought it was "not significant enough"? No indeed, that's right, that was never the intention:
"This pilot [...] is set up to provide a possible signal for the use of ivermectin in COVID-19, not to provide definitive evidence on the subject, hence the small sample size.”
Below as an example (spoiler alert, but you're not going to dig through the research anyway) six graphs from the study, each of which indicates in 28 days (the bars) how the symptoms progressed. The top row of charts indicates the results of the ivermectin group. The bottom row is the control group. The higher the bars, the sicker. I don't know... It seems that it does do something. The media, for inexplicable reasons, shows no interest in a drug that might reduce the severity of this "devastating pandemic" to that of a treatable flu-like virus.

As additional evidence against the effect of Ivermectin, I then receive a link to a LinkedIn post in which the above two studies are cited. I'll leave that one for what it is.
Argument 4: Ivermectin is more expensive than claimed
In this we find the price argument that Ivermectin is not that cheap at all. "about Eur 52 in total for a 'cure'!". And it is not reimbursed!
As if that price would remain the same with mass production on a global scale, and as if the remuneration would not be adjusted. The production costs of the drug are peanuts compared to vaccines. Not treating is ultimately even more expensive. There are countries where ivermectin is provided free of charge. I won't go into this any further, I think it's a strange argument when you know how many billions have been thrown away for measures and vaccines that no one knows the details of yet.
Argument 5: EMA also advises against
"The EMA therefore concluded that the use of ivermectin for the prevention or treatment of COVID-19 cannot currently be recommended outside of controlled clinical trials. More well-designed, randomized trials are needed to draw conclusions about whether the product is effective and safe in the prevention and treatment of COVID-19."
Another call for research. If you do not know how to organize such an RCT yourself, you will have to wait a long time and you are apparently willingly part of the commercial force fields in the pharmaceutical industry. This has yielded a lot in the past, but you can at least demand that governments and healthcare and (public) health institutes address gaps in the system. The ball is really in the court of the healthcare institutions and governments, and they just let the ball fall out of their hands.
"Not being able to recommend" sounds different from "against advising". Not being able to recommend wholeheartedly due to a lack of RCTs is completely justified. That the only solution is to impose a penalty of €150,000 on doctors for deregistering, that is mismanagement.
As an aside, I would like to note that the EMA still does not see a link between vaccine and blood clotting. That others have really announced that connection before I described on March 19th in response to the general amazement surrounding the phenomenon.
Argument 6: the side effects are serious
There are studies on serious neurological side effects of ivermectin. That sounds serious and for those involved it is. However, it concerns a few dozen cases after hundreds of millions of doses.
Serious Neurological Adverse Events after Ivermectin
Result of a other research, specifically aimed at administration of doses higher than standard:
"The systematic review identified six studies for inclusion, which revealed no differences in the number of individuals experiencing adverse events. A descriptive analysis of these clinical trials for a variety of indications showed no difference in the severity of adverse events between standard (up to 400 μg/kg) and higher doses of ivermectin. Organ system involvement showed only an increase in ocular events in the higher-dose group in one study for the treatment of onchocerciasis, all transient and mild to moderate in intensity."
Then also looked at WHO:
“Since ivermectin was used in humans, side effects occurred in 50% or more of the population (7) and ivermectin was 'contaminated' with a high side effect profile, despite evidence that most such reactions were due to the interaction between the drug and the disease, not the drug itself (8). A number of follow-up studies have found that the inadvertent use of ivermectin by filariasis on a large scale during pregnancy has not been associated with adverse pregnancy outcomes or negative effects on pregnant women or their offspring (9). The lack of serious adverse events found in the study reported by Heukelbach et al. is reassuring, as the low incidence of minor adverse events decreased from 14% after the first treatment to 5% 10 days later. “
The side effects cannot be a reason to prohibit doctors from prescribing. In countries where ivermectin OTC is available, accidents with overdoses happen when people do not receive the prescription through a doctor.
Interesting argument 7: It's the humidity!
[SPOILER: AIR HUMIDITY, TEMPERATURE, AVG. AGE, NOTHING CAME OUT OF THIS. Skip to Doing ]
Previous criticisms are based on repetitions of known positions and studies. For example, the aerosol theory has also been debunked for years. However, one of the criticisms stood out for me. As a reminder, it was a graph in which the correlation between Ivermectin use and Covid mortality is hard to deny:

Now, correlation does not just mean that there is also a causal relationship. For example, it may be that ivermectin use has a cause and that the lower mortality has the same cause. One of my own critical questions was therefore:
"The countries where Ivermectin is used may be less urbanized and therefore less susceptible (? Turns out not to be the case upon inquiry, but I'm not an Africa expert.)"
That is why I found this objection to make sense:
"Where ivermectin is used in Africa, it is generally a climate where there are many water features and therefore higher humidity. This is also a situation where a virus lives longer and therefore the chance of infection is greater and the consequences of a lung infection are greater. The population will therefore be more resistant to virus infection anyway due to more constant exposure."
I see a difficulty in this reasoning. If you turn it around, you can draw the same conclusion:
- Because there are many viruses in those (wet) areas anyway, people have a better resistance to the coronavirus. It is logical that corona mortality is lower there.
- In the (dry) areas where there are few viruses, the conditions are unfavourable for any virus, including the coronavirus. It is logical that corona mortality is lower there.
So the conclusion does not follow from the premises, there are still too many assumptions that you would have to prove.
For example, that viruses 'live' longer in high humidity. That could be an explanation, were it not for the fact that I have understood from scientific studies that viruses spread optimally at LOW humidity. Hmm...
The most dangerous humidity is below 40%. Above 60% and certainly above 80%, it becomes unclear what exactly is happening. In any case, the virus should have a hard time between 40% and 60%, the green area on the map below. Viruses flourish in low temperatures and little sun, but that is hardly to be found in Africa – at least during the day.

The green zone on the map is therefore the relatively "safe" zone. In the drier (red) and perhaps in the wetter zones (blue), the virus can spread better. And there too they have seasons that influence spread. If we have to go that way, it will be really terribly complex, too big and far too diverse with subclimates and so on. Someone else can dive into that.
Different approach.

The average relative humidity in African countries. For such a huge continent with a diversity of landscapes and temperatures, an average doesn't mean much. I looked at it anyway, looking for clues in that direction. Only in February is the average relative humidity in the safe zone. But it doesn't say much. So let's look at each country.
Humidity per country
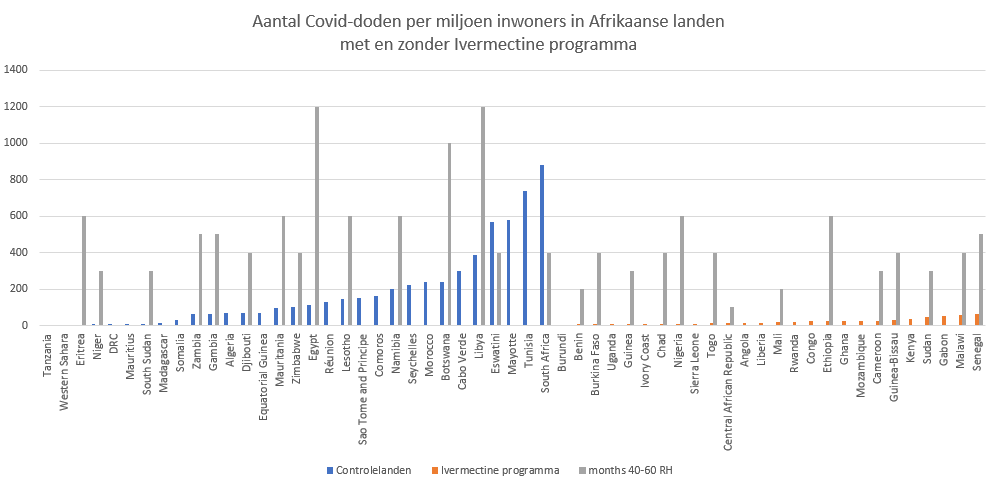
In the end, it's all about how it works per country. So the thesis is that the humidity in the ivermectin countries should be higher than in the other countries. Now that differs not only per area but also per season. To get an impression, I investigated how many months each country is in the safe zone of 40%-60%. That is low by African standards; Most countries have 0 months in which this occurs, they are always above, up to 90%. The gray bars indicate the number of months (divide the value by 100) that the relative humidity is between 40% and 60%. It does not seem to play a - or with some good will a very small - role.
Temperature per country
I don't give up that easily. The same exercise below again with average temperature of the countries (and in another source I saw that Lesotho should have 10 months instead of 6 months, sorry):
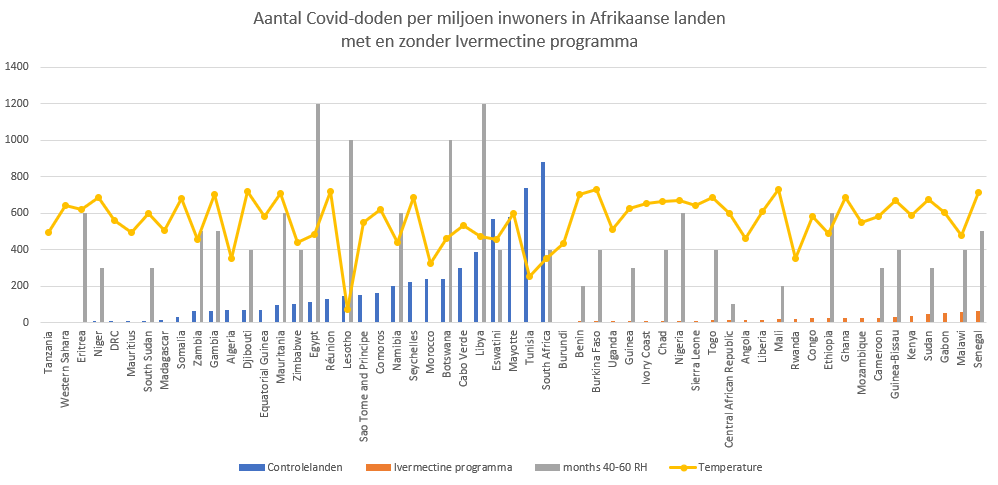
The four longest 'safe' periods are on the right side in the blue group. I find no support for the assumption that the mutual humidity makes a difference, in a positive or negative sense. So it's not that argument for me either... At least not without further explanation or substantiation.
What about life expectancy?
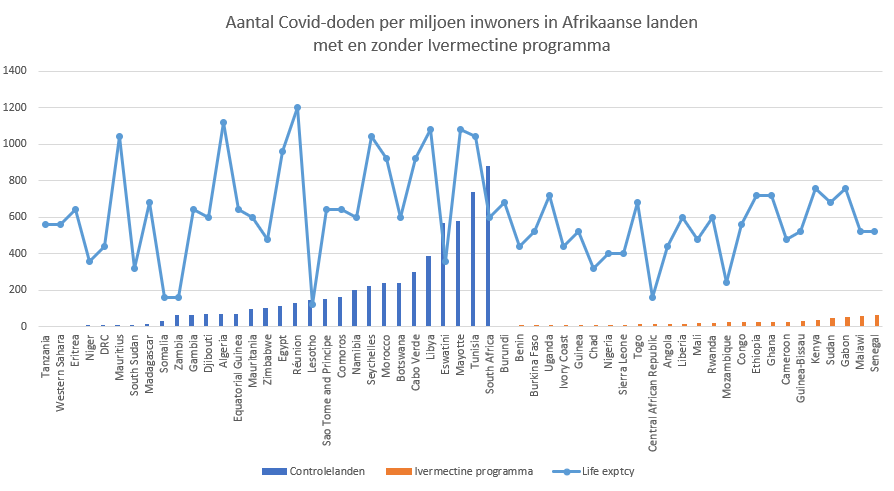
I also tried life expectancy. In a younger population, you can expect less mortality.
Blue has an average life expectancy of 67, orange of 63 years. (For orientation: lowest point of the line is 53, highest point is 78, I have enlarged the line to make a possible trend more visible.) River blindness reduces life expectancy by 8-12 years, I read on Nature.com. This is not in line with the known life expectancy (if IVM can be said to be the presence of river blindness; there are also malaria countries in between) So there are fewer people over 63 living in those areas. Could that be where the difference comes from? That's where the bulk of the dead is with us...
If you then look at each country, that is also a dead end. There are too many exceptions to make it a rule. Here you should use a statistical test to see if there is a connection between age and mortality. Both blue and orange seem to increase the light. I don't give it much of a chance.
In the process
New questions also arise:
- Brazil is also largely tropical rainforest (humid) and things are really not going well there. Which doesn't suit me at all because doctors do prescribe Ivermectin for that... There may be other factors at play such as
- Obesity, unhealthy eating is a problem in many South American countries – perhaps a vaccine will help better in such a susceptibility and high-risk group.
- A water-rich environment in the blood heat, does that automatically mean high relative humidity?
- There are certainly many countries in Africa where the conditions are so unfavorable that you cannot grow old without a strong constitution, while here you can continue in a nursing home for decades. But isn't that the case in the non-ivermectin countries? Poor food and malnutrition, water shortages? Lower life expectancy means less Covid mortality? Maybe something to figure out, but I wouldn't see anything striking soon.
- If you are trained to survive parasites, malaria mosquitoes, bacteria, polluted water, rotten food, no food or drink, overheating, biting dust – do you automatically have an immune system that resists respiratory viruses better? Or are you weakened so that you are more likely to die?
websites with overviews of ivermectin studies
Closing speech
I completely understand the continuing dismissal of so many positive signals under the protocol motto "not significant" from a scientific point of view. In a crisis situation, however, I do not think it is responsible to keep saying "we are waiting for a large RCT". There are too many cries for help from all regions of the medical world. Someone has to take action, right? Help dispel the fable and show why everyone was mistaken, or convincingly prove that it is an important medicine in the corona fight.
A fundamental problem is that such research should be carried out independently. The major parties that can organize an RCT are all interested. The WHO wants to vaccinate. The governments have stuck their necks out with blind investments of millions in vaccine development; They are not going to drop the chopping block themselves. The producer of Ivermectin itself has an interest in vaccination. The other pharmaceutical companies have no interest in a patent-free competitor for the annual global vaccination campaigns that lie ahead. Independent doctors cannot afford it and perhaps they too are too biased to be able to set up or carry out such an RCT properly. In short: we are stuck. What then? Call on the Swedes for help?
If I only look at the Netherlands, we are full of healthcare institutes, health authorities, patient associations, interest groups. For example, we have "The National Health Care Institute monitors on behalf of the government whether our care is and remains good and affordable." I haven't heard them yet in the past year. Shouldn't they sound the alarm? Or "ZonMw funds health research and stimulates innovation in healthcare." A government agency that apparently has a low-profile strategy. Where have all those health watchdogs and budget guards gone? Why don't we hear anyone from the "Domain of Quality of Care"?