
Clear causal link between mortality and Covid vaccine rollout
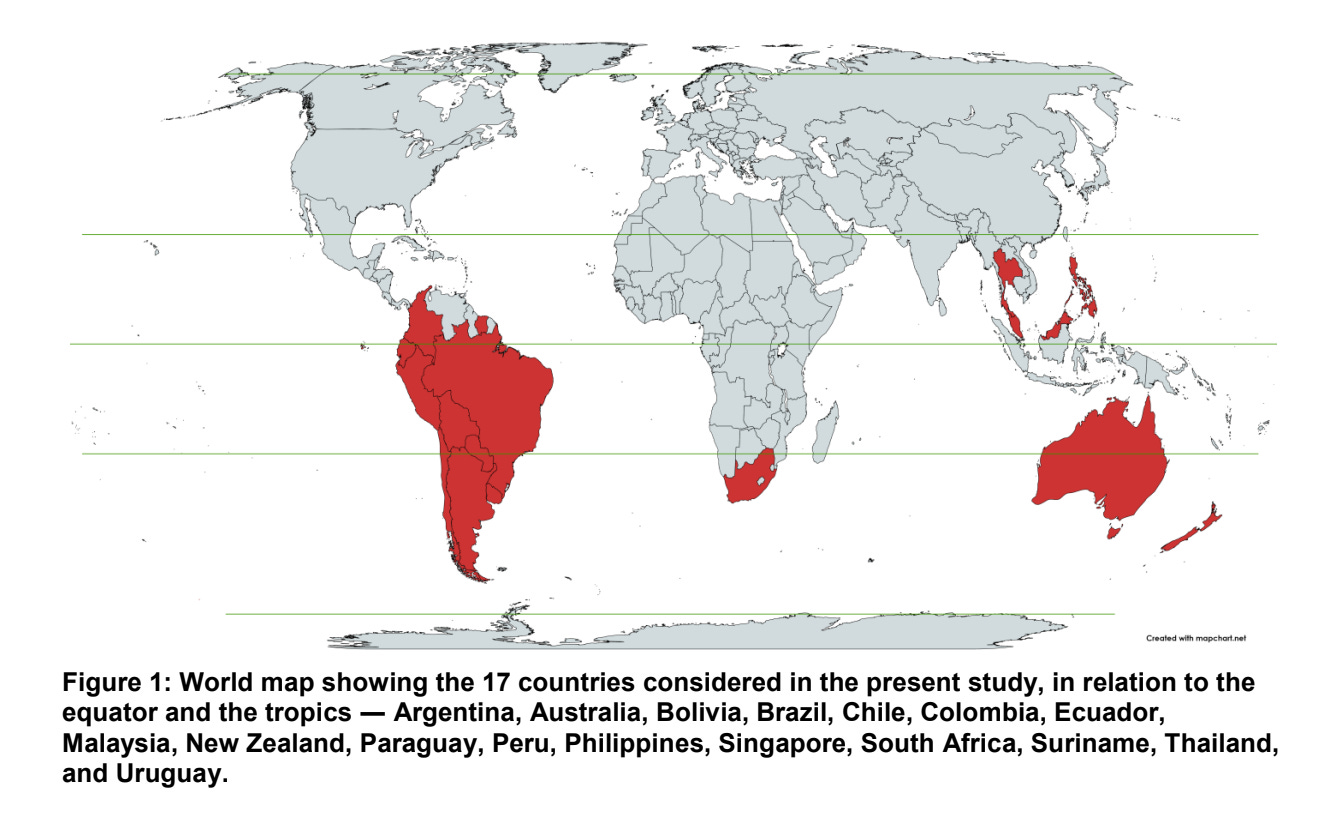
What Byram Bridle was already beating the drum about in May 2021 is now, three years later, also the outspoken position of a new article by Denis Rancourt et al (180 pages), which analyzes all-cause mortality (ACM) in 17 countries in the Southern Hemisphere and in the equatorial region. The authors find a "clear causal relationship" between spikes in All-Cause Mortality (ACM) and the rapid rollout of vaccines across four continents.
I read it, wanted to devote an article to it and then saw that Rebekah Barnett already a fine one Summarizesg . This is my adaptation of it, including some additions on my part.
"The COVID-19 vaccines do not save lives and turn out to be deadly toxic substances."
The not yet peer-reviewed article by Denis Rancourt et al. attempts to quantify the risk of lethal toxicity by injection, which "appears to be extraordinarily high in most elderly people". The authors conclude that "governments should immediately end policies of prioritizing older people for COVID-19 injection." This is based on public figures from 17 countries in the southern hemisphere.
All-cause mortality: the ultimate vaccine test
In the summer of 2021, it was clear that the persistent excess mortality did not match the promise of the vaccinations. ACM (mortality from all causes) is the final bill: if it is far too high, something is not right at all. As an epidemiologist, someone like Christine Stabell Benn has always been keen to compare the ACM of vaccinated people with that of unvaccinated people. It has also been a reason to withdraw effective vaccines: it helped well against a certain disease, but jabbed people died more often from other things than before from the disease. The WHO also sets this mortality requirement on paper for vaccines. Only not now because it is an emergency situation.
The data for thorough analyses must come from the government, but they do not deliver, they do watch out. Rancourt et al. therefore have to rely on ACM mortality peaks at population level in several countries, from public sources that vary greatly from country to country. Whatever we have instigated on virus varia, which Herman Steigstra has energetically addressed.
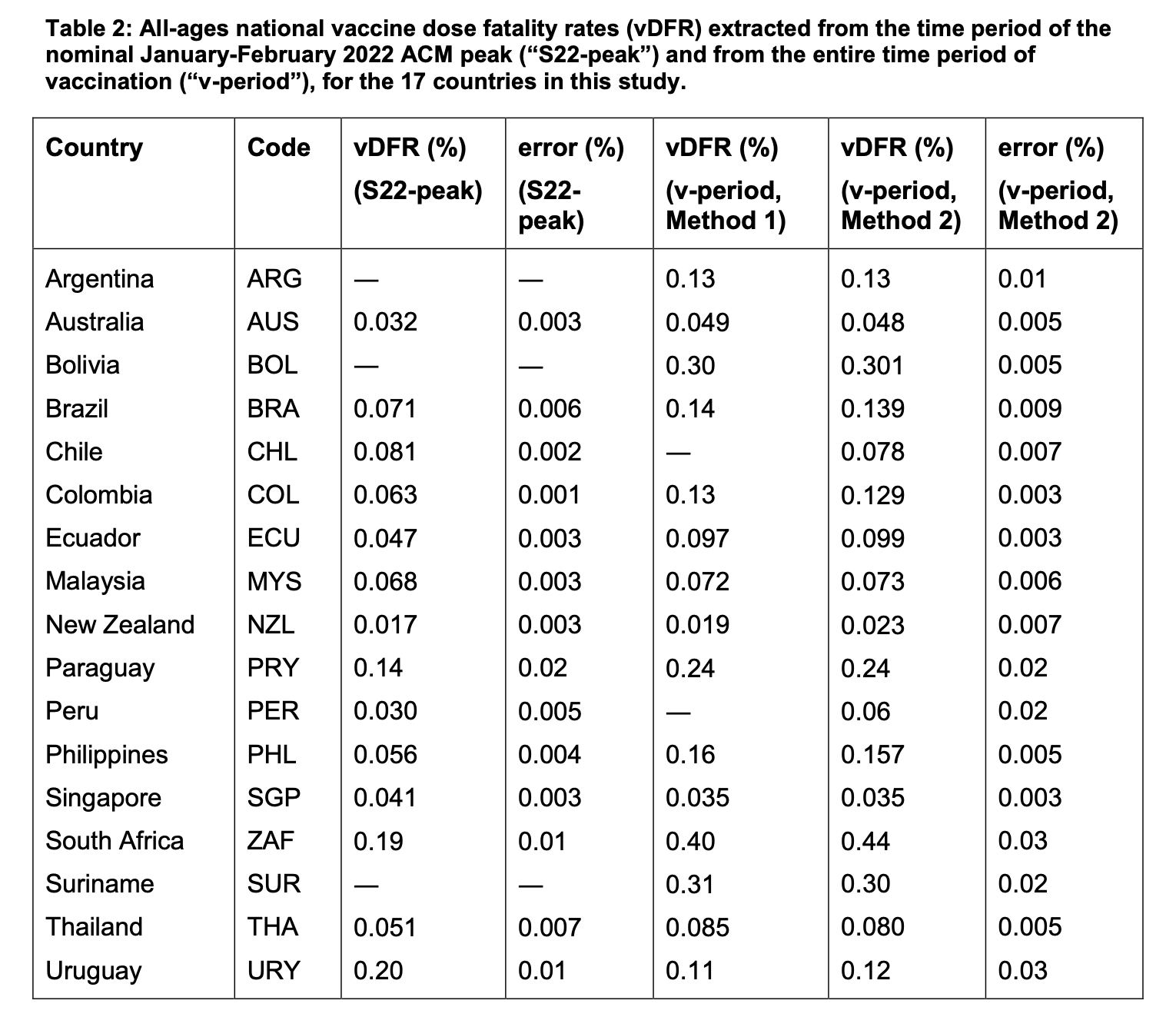
Vaccine-dose fatality rate (vDFR)
The authors calculated the mortality rate from vaccination and arrived at about 0.05% (1 death per 2,000 injections). This number increases exponentially with age: the vDFR doubles with every five years of additional age, to about 1% for people aged 80 and older.
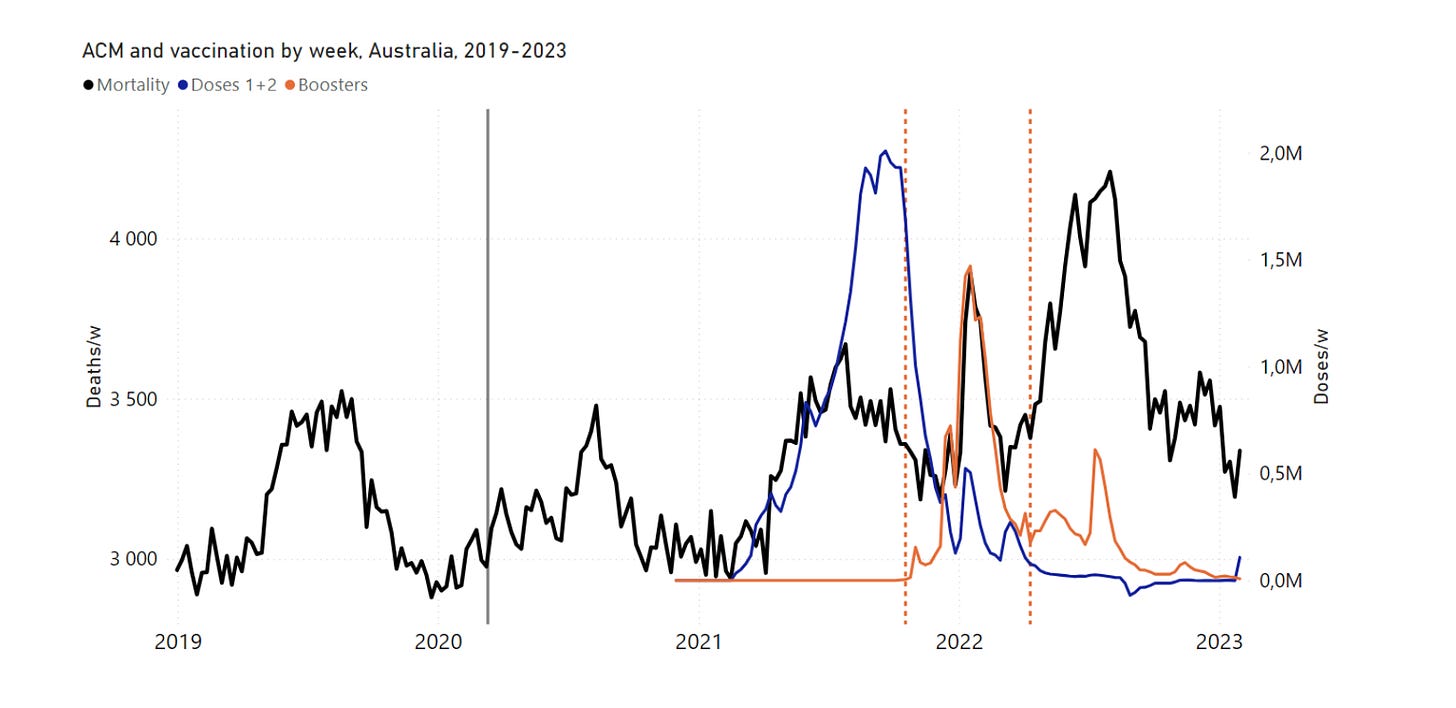
Australia
One could argue that for the Australian analysis, the sharp spike in ACM coincides with the initial spread of Covid across the population (especially in Western Australia, Queensland, and South Australia) and that these deaths are therefore Covid deaths. Rebekah also believes that Rancourt has not convincingly dismissed this counter-argument in his previous articles on Australian ACM.
What is not in her own summary is that Rancourt also explains in the presentation that it is impossible for a disease wave to break out everywhere in the world at exactly the same time. For him, this is an important basis for the statement that 'it can't be a virus, it can't do that'.
But it is clear that Australia and New Zealand were much later, while Rancourt says that it reared its head everywhere at the same time, how does he reconcile that? Of course: islands may have different laws when it comes to viruses blowing over – but it wasn't because of a virus, was it? He needs to explain that better.
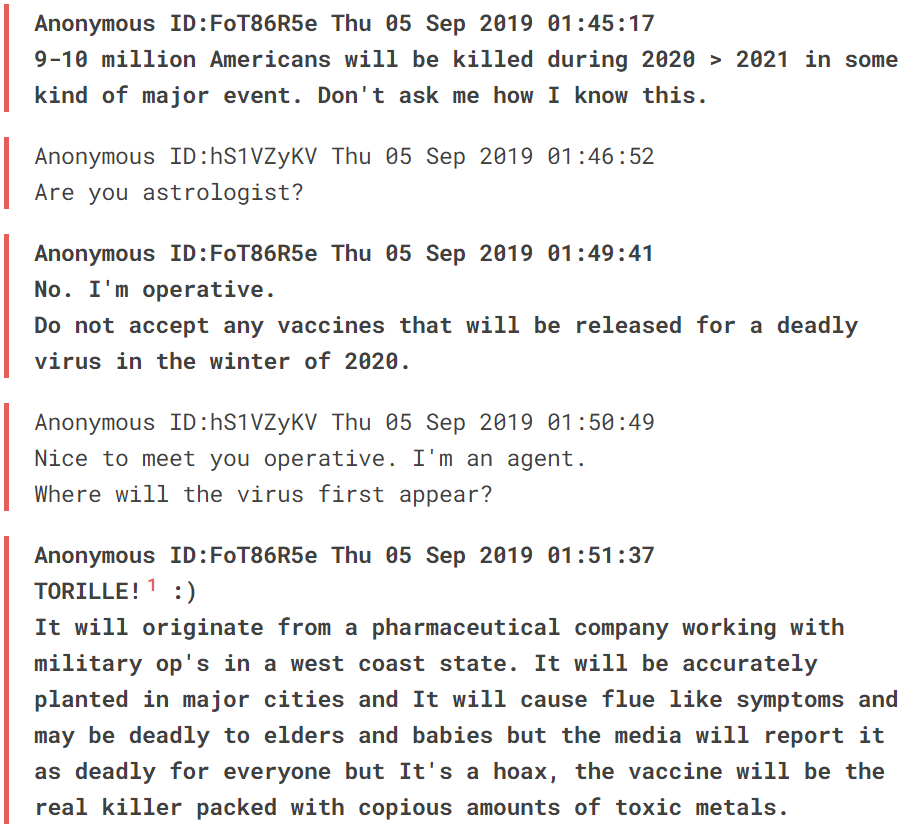
In any case, Rancourt does not appear to be a sinister conspiracy theorist here, otherwise he would have mentioned another option. An 'Anonymous' predicted quite exactly what would happen in 2019. For a conspiracy theorist, this would be sufficient evidence to assume planning.
(this message is also in the Wayback Machine on that date, so it was not manufactured afterwards).
An analysis of Queensland's mortality rates by Dr Andrew Madry shows that the upward trend in ACM began with the rollout of the primary series and nine months before the spread of Covid in the community. Yet Rancourt holds "the measures" largely responsible here, while those very strict measures in New Zealand and Australia have not had that effect.
It is clear that the vaccines also turned out to be disastrous in Australia. His points:
- Most Covid deaths in Queensland were fully vaccinated (and some boosted) when state borders first opened in December 2021/January 2022;
- Excess mortality began in 2021 when the vaccine rollout was in full swing, but many states did not have Covid;
- Unprecedented high rates of adverse event reports when most of the population was vaccinated and there was no Covid. More than half of those who reported an adverse event reported to the hospital, which gives an idea of the severity of the side effects.
- Data from New South Wales show that those with more doses of vaccination with Covid were more likely to die or present in hospital and ICU than those with 0-2 doses. The answer to this is possible: "the older, the more often you are vaccinated". Is that true? The data is not age-stratified and no one from the Ministry of Health has been able or willing to demonstrate effectiveness by publishing the full age-stratified data. In fact, they bend over backwards not to do this, just like with us in the Netherlands.
- A Bradford Hill analysis of the Australian ACM by analyst Dr Wilson Sy, from which he concluded: "Strength of the correlation, consistency, specificity, temporality and dose-response relationship are the main Bradford Hill criteria that the data meet. This suggests that the Australian pandemic is indeed iatrogenic, with excess mortality largely caused by COVID-19 injections."
The common thread:
"In 9 out of 17 countries, there is no detectable excess mortality until the vaccines are rolled out [...] In the other 8 of the 17 countries, a new regimen of higher mortality will be initiated after March 11, 2020 and prior to each administration of the COVID-19 vaccine
In all 17 countries, vaccination is associated with a regimen of high mortality, and there is no relationship over time between COVID-19 vaccination and proportional reduction of ACM."
[By this he means that the average mortality is slightly increased, so for example also in the summer. How does that work, that mortality goes up before vaccination, medo 2020...? Typically a problem that arises when you try to rely only on ACM. You will still want to compensate for an underlying flu wave and before you know it you are again working on a baseline from which you derive the increase and decrease mortality in order to arrive with/through corona.]
There are many graphs with temporal correlations. They are all variations of the below, for all 17 countries, with different methods of analysis. I don't find them all equally convincing.

In some graphs I see something different from what Rancourt gets out of it. Example: Peru, the country with the most Covid deaths per million inhabitants. He links vaccination to mortality. But people died before the vaccination was taken. The first two death waves in particular stand out in the blue line. So Covid was indeed either serious or, for example, antibiotics were no longer given to lung and respiratory patients. Covid was not seen as such either: "we didn't know anything about it" so it wasn't treated adequately, that wasn't even possible. But vaccination (orange) only came after that. I get the feeling that the "1-year moving average" is a way to get vaccination and mortality on top of each other. "Associated with" it is called.
Another graph is this one showing a correlation between countries with more jabs and higher mortality versus countries with fewer jabs and lower mortality.
As we have already figured out, that is a meaningless graph. You should also make this mortality comparison for 2020 or even earlier. What did the mortality ranking look like at the time, did it differ between countries where there would be little and a lot of vaccination later on? Has that vaccination changed anything in those relationships? In any case, no positive effect was discernible in Europe.

Criteria for causality
According to the authors, their analysis more than meets the "robust criteria" laid out by legendary scientist John Ioannidis:
“Experiment: The same phenomenon is observed independently in different jurisdictions, for different age groups, and at different times, which constitutes sufficient verification in independent large-scale experiments in the real world.
“Temporality: The many incremental increases and abnormal peaks in ACM are synchronous with the rollout of vaccines; Even in jurisdictions where excess mortality only occurred after about a year after the declared pandemic until the vaccination was implemented.
“Consistence: The phenomenon is qualitatively the same and of similar magnitude every time it is observed."
Therefore, "there can be little doubt that the mass COVID-19 vaccination campaigns caused the temporally associated excess mortality in the 17 countries of the current study, and in other countries studied so far," according to Rancourt et al.
Evidence for causal link between vaccines and ACM surges
The authors refer to a plethora of evidence supporting a causal link between vaccine rollouts and ACM spikes:
- Autopsies. One systematic review of 325 autopsies following deaths related to Covid vaccination up to May 18, 2023 showed that "a total of 240 deaths (73.9%) were independently assessed as directly attributable to or significantly contributed by COVID-19 vaccination."
- Studies by Vaccination-induced pathologies
- An established causal link with pathology caused by vaccination, based on histopathological and immunohistochemical staining of skin biopsy samples
- Secondary analysis of serious adverse events reported in placebo-controlled, industry phase III randomized clinical trials
- More than 1,250 peer-reviewed publicationss about side effects of COVID-19 vaccine
- The known vaccine compensation programs of states around the world, including deaths from the COVID-19 vaccines
While the above does not prove causality on its own, but rather demonstrates plausible mechanisms and circumstances, the authors provide the following to demonstrate the causal relationship. This link is made in several studies at the population level:
- One overview study by Mark Skidmore, which was later Withdrawn under heavy pressure on the editors of the journal by parties who were not happy with his conclusion: "With this research data, the total number of fatalities due to COVID-19 inoculation can rise to 278,000 when fatalities that may have occurred without inoculation are removed". [I have to say that I didn't see much in it even then]
- Previous quantitative evaluations of vaccination dose mortality (vDFR) based on all-cause mortality (ACM) data in different countries (Rancourt, 2022; Rancourt et al., 2022a, 2022b, 2023) (View Rancourt's papers here)
"These findings are compelling. The associations are numerous and systematic and there are no counterexamples. In our extensive investigation into ACM, we found no evidence that COVID-19 vaccines had a beneficial effect."
Denis Rancourt et al.
Tackling counterarguments
The authors refute several counterarguments, including that the ACM peaks are caused by
- Seasonal effects
- heat waves
- Earthquakes
- other aggressive Covid countermeasures
- underlying health conditions
- Covid infections.
[I still miss the climate in this list]
So there are a few things to criticize, but they do make a point that Covid itself cannot have been the driving force behind ACM:
"Regarding the theory of the emergence of one or more variants of SARS-CoV-2, this emergence should cause simultaneous peaks and peaks of mortality in 17 countries spread over 4 continents (Figure 1, Figure 2, Figure 4, Figure 11, Figure 14, Figure 18), which is statistically impossible if we accept the theories of spontaneous viral mutations and contact spread of viral respiratory diseases; and all the resulting spikes in mortality would have the remarkable coincidence that they occurred exactly at the time that vaccination boosters were being rolled out."
'Vaccines have saved 20 million lives'
Believers in Covid vaccine modeling will throw their hands up at this point and shout, 'but Covid vaccines saved 20 million lives! Of course, the ACM has risen, but Without the vaccines, it would all have been much worse'.
Rancourt et al. rightly do not waste many words on this. The model calculation has often been wrong by a factor of 40 (and more). The effects of natural immunity were overlooked, the vaccines were supposed to be highly effective. Many articles have already been written about this, such as this from Brownstone.
They do mention the argument that a study in 108 countries found that those with the highest Covid vaccination rates also had the highest Covid death rates, while the reverse was true for countries with low Covid vaccination rates. [We have already done that (thanks to Herman) better contradicted].
Incorrect data underestimate harmfulness
The authors suggest that the discrepancy between their findings and the official Covid data reported by governments and related regulatory agencies is because "the monitoring of adverse events, the reports of clinical trials, and the statistics of death certificates greatly underestimate the lethal toxicity of the injections".
Joel Smalley has reported extensively on the situation in Australia and what is going wrong there. I recognize a lot of what is happening on the other side of the planet:
- There is a double standard when attributing deaths to Covid [the same WHO guideline applies as the one we have complained about here before].
- Underreporting that is not included in any official publication
- Not a good follow-up of reported injuries and deaths
- Autopsy not encouraged for post-vaccination deaths
- No active monitoring tests for Subclinical damage
- Medical censorship means that medical professionals are not only inadequately trained but also strongly discouraged from properly diagnosing and reporting vaccination injuries
There is also evidence of death code tampering that inflates Covid deaths and hides vaccine deaths. For example, the miscoding of vaccine deaths in Minnesota led to accusations of "data fraud" against the CDC.
Two waves of injuries and deaths
Last week, cardiologist, internist and epidemiologist Dr Peter McCullough said in a speech to the European Parliament [last week we already noted that that was not a speech to the European Parliament, but OK]:
"There have been two waves of damage in the world. The first was the SARS-CoV-2 infection, which was at the expense of the weak and elderly. And the second wave is now the COVID-19 vaccines."
Watch Dr. McCullough's full speech to the European Parliament on 13 September 2023 (17 min)
One explanation for the two waves is the phenomenon of 'spikeopathy', as Jillis Kriek described it on this site in December 2022 in 'What Covid 19 and mRNA vaccines have in common‘. Later, in June 2023, it was explained in a peer-reviewed article in the journal Biomedicines, titled 'Spikeopathy': COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA. 'Spikeopathy' refers to the toxic effects of the spike protein, whether it comes from the SARS-CoV-2 virus or is produced by gene codes in mRNA and adenovector DNA vaccines.
In addition, the mRNA vaccines also introduce lipid nanoparticles (LNPs) into the body, which are themselves pro-inflammatory and carry the spike-producing mRNA to parts of the body where the viral spike protein does not normally end up.
Dr McCullough has previously suggested that taking Covid 'vaccinations' increases the risk of damage due to exposure to spikes . He suggests limiting exposure to spikes by avoiding the injections and nasal rinses as a prophylactic.
I sense a heavy bias in Rancourt's piece. He focuses exclusively on vaccine damage and sees deaths from Covid as fairly normal seasonal mortality. I'm more in line with Dr. McCullough. Covid was no sweetheart and has caused a wave of injury and death – although to a lesser extent than the vaccine and also far less than all the measures that resulted in the declaration of official panic status, which also prevented Covid from being treated in an effective way. What mortality would have looked like without the accumulation of policy errors will always remain a point of discussion.
Either way, Rancourt and McCullough draw the same conclusion – the only appropriate response is to stop jabbing.
Question for readers who would like to participate:
How do you explain the existence of datasets/analyses that seem to directly contradict Rancourt's findings, such as this analysis by ACM In several countries where the author believes that the vaccines have been beneficial?
Conclusion
With admiration for the hard work, I am afraid that Rancourt has allowed himself to be carried away in his consternation. That is very understandable because it is appalling what has taken place. The system has become corrupted from top to bottom (but especially above) under pressure from what is going on in a global market of hundreds of billions.
The reality is more diverse, more dynamic and therefore much more complex than he tries to imagine. In that simplification process, valid critical questions sometimes lapse. That is a pity, the scientific tone regularly swings towards activism that does not tolerate contradiction.
*Rancourt is no longer bothered by any peer review process and publishes directly on his website. There are advantages and disadvantages to this, but in the current climate, in which the Integrity of medical journals disappears and activist journalists and academics successfully lobby for the retraction of research they don't like, rather than honouring the scholarly tradition of debate, it's understandable that some researchers simply quit.
Denis Rancourt therefore no longer sees any benefit in the peer review process. In my opinion, his piece could be greatly improved – with the right peers.
All the graphs make me a bit red-eyed. And the reality does indeed seem even more complicated.
An important fact that has contributed (still contributes?) to the high mortality (due to or with Covid) is the ban on treatment. In your article you mention antibiotics. Pneumonia, triggered by a virus, can eventually turn into a bacterial infection. And a traditional antibiotic treatment would offer relief. In addition, the bans on hydroxychloroquine and ivermectin on pain of deprivation of the license. That cost many lives.
I'm glad I never took one of these shots. As far as I'm concerned, there is more than enough evidence that the whole approach has backfired, to put it euphemistically. The fact that it is not recognized in the MSM, and that 80% of the population believes the story of the 20 million lives saved is a problem. Although I recently saw 15 million pass by (also without any substantiation).
That is the key question for me now. Not the question WHETHER the measures taken (including the Non-Medical Interventions such as lockdowns etc.) were harmful. That is obvious. I would like to understand the origin of the madness, at the risk of diving into conspiracies. If we now assume (for arguments sake) that the measures are as catastrophic as we assume, then the question remains whether it was set in motion consciously or unconsciously.
If I put everything together (and that in itself is quite a task), then there has been deliberate manipulation, very bad choices have been made with regard to health care, with catastrophic consequences for the global economy, among other things.
There has been a 100% bet on 'vaccines' that have cost governments billions. Could it really only be about turnover from the pharmaceutical companies? Who, by the way, have a big finger in the pie with agencies such as CDC and EMA. Could it be so banal? And that the rest of the developments resulted from the spasmodic clinging to the narrative?
I think that various parties had hoped for a continuous contraction of the world economy in which climate goals could be achieved. So then you abuse a crisis to achieve other goals. To claim that the virus was deliberately created is going too far for me. That it was caused by a lab leak is now the most plausible scenario. That it was then covered up is also clear.
I no longer believe it was inability. But what then? And why is it (Mattias de Smet answers this) that so few people are skeptical?
Nuance is somewhat lost and local variations remain out of the picture, but Rancourt's approach is certainly refreshing.
For example, the benefits of measures to ACM depend on specific local circumstances and customs.
Or e.g. people with a positive Covid test
are not treated for potential pneumonia, but that they are put on the ventilator when it has gotten out of hand, which can be seen as iatrogenic action in retrospect, depends on: whether one has tests and then whether there are people who can be tested positive, whether one pursues a withholding hospitalization policy because of fear of capacity problems, they have access to ventilators, they have enough staff in the hospital and last but not least they think that ventilators where heavy people are intubated on the ventilator in a prone position work.
In Germany there was sufficient staff and capacity and there was little in the way of treatment with ventilators.
In Italy there was a shortage of staff and an oversupply, and no holding off policy and I think it was decided to put several people on a fan.
These countries gave huge differences in ACM in the pre-vaccination covid year.
In Australia, due to isolation in the same period, people with a positive test were lacking
and did not pose these risks of potential iatrogenic damage. Less was died (but also not lived).
I don't know the situation in Peru. You would say that not knowing that people were testing positive, no iatrogenic damage could take place in the way described above.
Definitely deserves further investigation.
Analysis of local working methods and circumstances can only help us further.
It is all the more reprehensible that WHO, as a know-it-all, seems to be striving in advance for a coercive one-fits-all approach.
PS. I suspect that in respiratory problems, factors of air pollution and the more favorable conditions for all kinds of harmful aerosols penetrating deep into the respiratory organs also play an important role in the respiratory system, in combination with a decrease in D supply and a related reduction in immunity at the end of winter.
It's nice that you give a Dutch adaptation of the article. With all due respect to you, I think it's a bit of a weak conclusion. Of course it is complex, and peer-reviewed is better. That's true for any article about this draft, right? The challenge you give your readers is now returned, so that you can really add some "opinion and science columns" :).
I couldn't make more of it this time. That happens sometimes, for what it's worth...