
The normal, average weight of people has always been approximately the target weight. The 'norm'. You could be too fat or too thin, but most people had a normal BMI, the word says it all. You can see it in old beach photos: fat people were exceptions. That is no longer the case. Nowadays most people are overweight: being overweight has become 'normal'. The 'normal' weight of that time (approx. 1970?) is still the target weight today, despite the fact that more than half of people are now overweight (CBS). 'Normal' has therefore not been elevated to a 'norm'.
Er worden vanuit de samenleving pogingen ondernomen om overgewicht te romantiseren met goed gevulde blije dames: "je lichaam accepteren hoe het is" en "trots te zijn op hoe je bent". Chubby fotomodellen geven het gevoel dat het OK is om te zwaar te zijn. Overgewicht moet net zo acceptabel en zelfs net zo gewenst worden als een sixpack. Alle mensen zijn immers gelijk.
However, science points out that being overweight is unhealthy and is associated with significant physical and psychological complaints and diseases. A study in The Lancet, with nearly 4 million participants across four continents, found that being overweight or obese increases the risk of premature death. People who are moderately overweight lose about three years of their life expectancy. Research from the University of Oxford found that too, plus severe obesity (BMI of 40 to 50) shortens life expectancy by about 10 years.
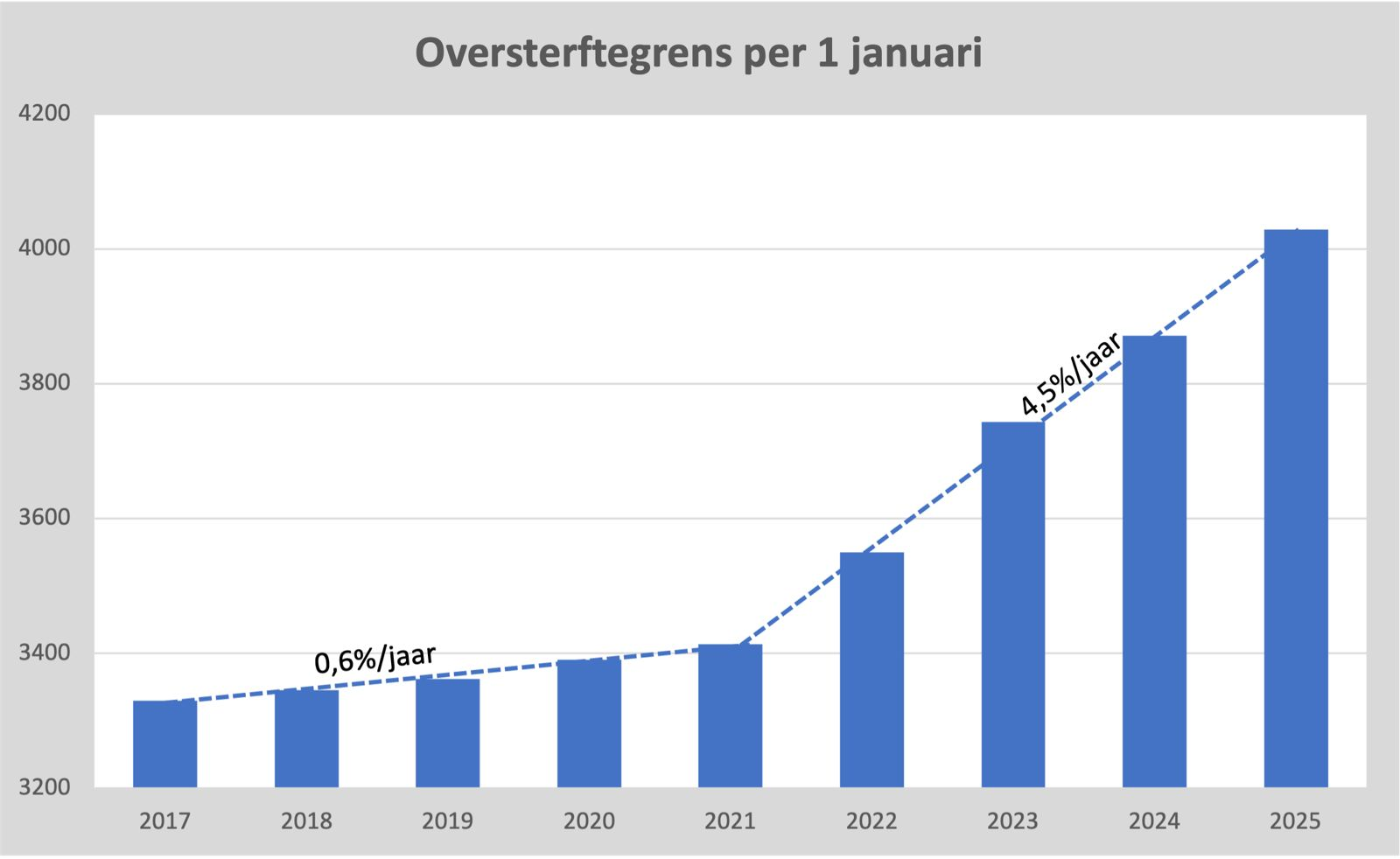
De wetenschap neemt ontwikkelingen in gemiddeld lichaamsgewicht dus niet mee in de definitie van "overgewicht". Een belangrijk en hard argument is dat een hoger lichaamsgewicht leidt tot hogere sterftekansen. Vandaar de term "streefgewicht", het gezond geachte gewicht dat aanzienlijk lager ligt dan het verwachte gemiddelde gewicht van 2024.
This is also part of the tasks of public health guards: indicating areas for improvement. Increased mortality is a merciless, rock-solid criterion.
Excess mortality as the norm
While the mortality rate is a strong argument to emphasize the seriousness of the subject of 'obesity', mortality rates themselves work very differently. Here too, average life expectancy was always the norm. In the event of a sudden change in mortality age, health scientists should bounce back: what is going on here, how is this possible? And if it worsens: how do we stop this? What should we go back to, what is a good reference? However, that doesn't happen. To everyone's surprise, the average is elevated to the norm.
"Ja natuurlijk", zegt iedereen met het brein van een olienootje, "de baseline wordt nu eenmaal sinds jaar en dag bepaald op basis van de sterfte van afgelopen jaren."
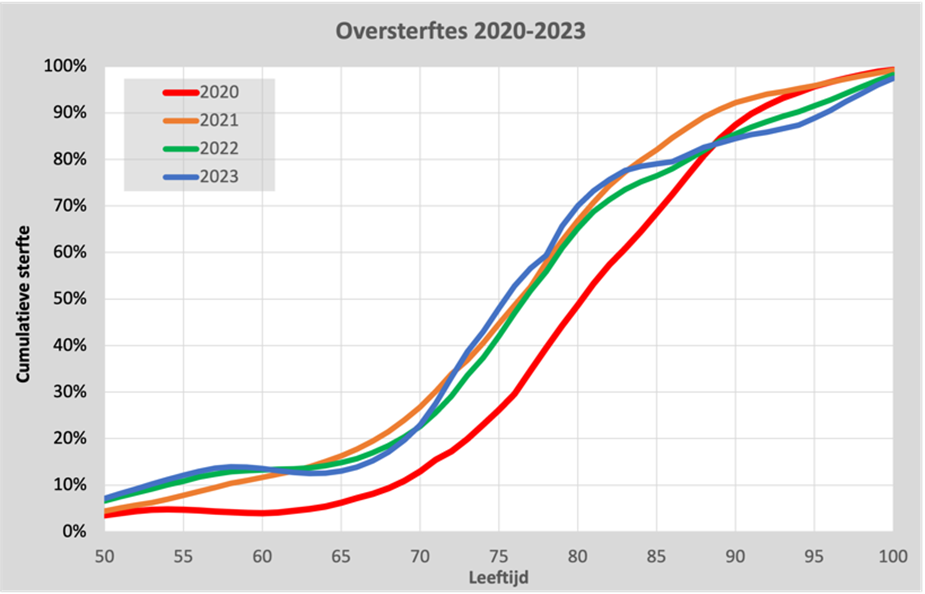
We see that in the excess mortality years since 2021, the age of mortality has been brought forward considerably. In 2023, a 75-year-old has the same mortality risk as an 80-year-old in 2020.
Als we dat simpelweg accepteren, wordt de norm verhoogd naar het hogere sterfteniveau. Wat we in 2020 nog oversterfte noemden, wordt nu "verwachte sterfte".
Hogere sterfte wordt genormaliseerd zonder oorzakelijke verklaring. De trend is kennelijk onomkeerbaar en er is geen behoefte om uit te zoeken of we niet terug kunnen naar het niveau van 2020 of eerder. We kennen geen "streefsterfte", zoals we wel "streefgewicht" in het leven hebben geroepen. De lopende trend wordt gewoon gevolgd en "verwacht". Oversterfte verdampt. Waarom zou iemand dat willen?
Excess mortality: fine, as long as it's not so hot
It is common to write off excess mortality as soon as we understand the cause. A heat wave, for example, is a fact of life that we will have to accept. But it is also an undesirable incident: reason to keep a close eye on it. Heat waves are therefore not included in the mortality forecast. In this way, we keep the baseline tight and incidental increases remain more visible.
As long as we keep the 'excess mortality' visible since 2021, this would indicate to us that the cause for that special increase in mortality is missing: we do not know what is killing us.
The sore point is that the increase started at the same time as the corona vaccinations, almost worldwide. This gives the impression that these vaccinations have been the biggest medical mistake ever. That means quite a bit: the industry would then have focused purely on profit, delegated responsibilities to governments that pretend to know nothing, Van der Leyen has simultaneously siphoned off vaccine billions via text messages, regulators have proven to be completely useless, experts have proven to be incompetent, journalists have been bought or simpletons (or both), science magazines turn out to be money laundering flyers, tower blocks with civil servants have meant absolutely NOTHING but zero point zero, doctors... etc., I'm not going to repeat the whole story of the - in that case - deeply corrupted system.
In any case, the vaccine industry will have to be thoroughly vetted - perhaps the entire medical-pharmaceutical complex - to justify blind acceptance of vaccines. The intensive supervision must be overhauled. The government can no longer be trusted. Government expertise must be organized differently. In short: it has quite a few implications. But the government would not be the government if the most important implication were not the 'willingness to vaccinate'. Because the health of the population comes first, it comes first! Do you understand?
Fortunately, vaccine damage is extremely, extremely rare, especially according to Lareb. A laundry list of side effects, from neurological to cardiological to respiratory, paralysis, spinal cord inflammation, organ inflammation, cancer, you name it, but they have one thing in common: one side effect is much rarer than the other, seriously. So you never don't get it. And look: only 600 deaths reported to Lareb! That's not even two MH17s. (And that's almost only during the jab campaigns.)
Lareb does a good job, they cover up these complaints in category cover-ups and thus keep them a bit sub rosa. They act like a rented call center to keep customers at a distance. But yes, that doesn't change the whining about that damned excess mortality... How do we get rid of that?
We have to consider it 'normal' that more people are dying since the injection campaigns. Then it won't help if we keep talking about 'excess mortality'. It is reminiscent of the problems with 'repopulation': that our population is changing in composition, that traditions are disappearing, that the national character is being multiculturally immigrated, that is not the point of discussion. The point is that we stop naming it. What you don't talk about doesn't exist.
Without target mortality there is no excess mortality and without excess mortality there is really nothing wrong, not even with the vaccines. No one really notices, only the funeral industry. If we just expect the increased mortality, there won't even be excess mortality. Trust in the government and therefore especially the willingness to vaccinate will remain intact.
De missie lijkt duidelijk: "Niets nalaten om te voorkomen dat de vaccinatiebereidheid daalt." Zien we daar meer signalen van? Zeker. Hieronder zet ik er een aantal op een rijtje. Al deze punten hebben gemeen dat ze vaccinaties uit de wind houden, met een focus op het laten verdampen van oversterfte:
- Denying immunity
- Tempering excess mortality in accounting
- Recalculate margins
- Definition nudging
- Lie
- Corrupted data (communication)
- Tweaking historical figures: falsification of history
None of this has anything to do with science or public health. But the seriousness of the offences shows that there are important interests involved.
Bias towards vaccination readiness
Recent examples, a selection from last month's harvest.
Vaccination is still necessary
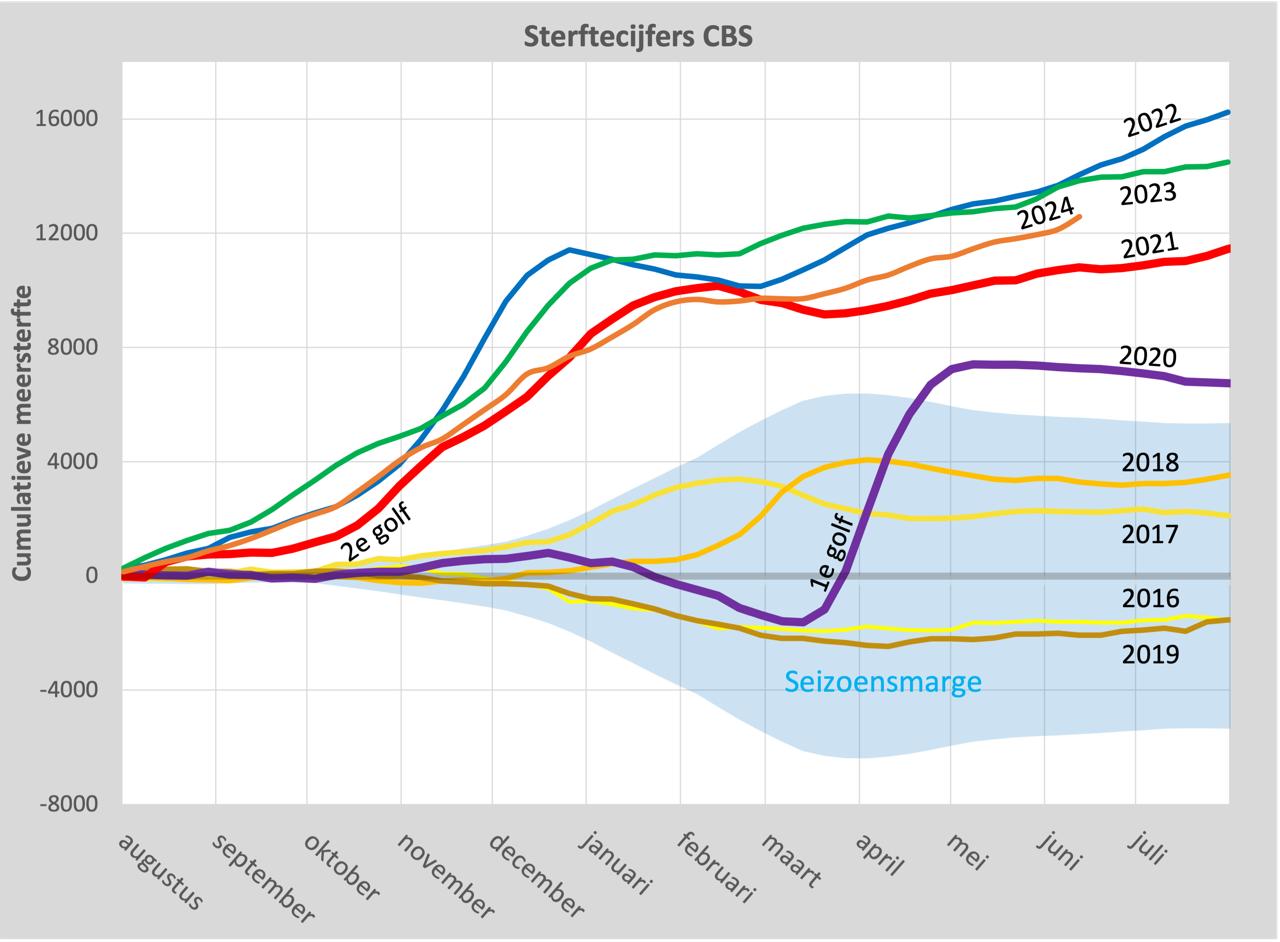
To make the overall bias explicit: at the beginning of July, RIVM removed the sentence marked in yellow, which truthfully states that those who have had a corona infection normally no longer need a vaccination. We don't know why that sentence was there for about a month (it was added in May), but we don't know anymore. In any case, one of the effects is that people who do not need a jab are not deterred from getting one. These are substantial extra points for the willingness to vaccinate in the Netherlands.

The prick-oriented approach is explicitly professed and shouted from the rooftops.
Excess mortality is tempered from an accounting point of view
In the past few weeks I have had a lot of contact with Herman Steigstra in connection with a piece on Researchgate about the increased expectation with associated bandwidth. A higher baseline results in less excess mortality.
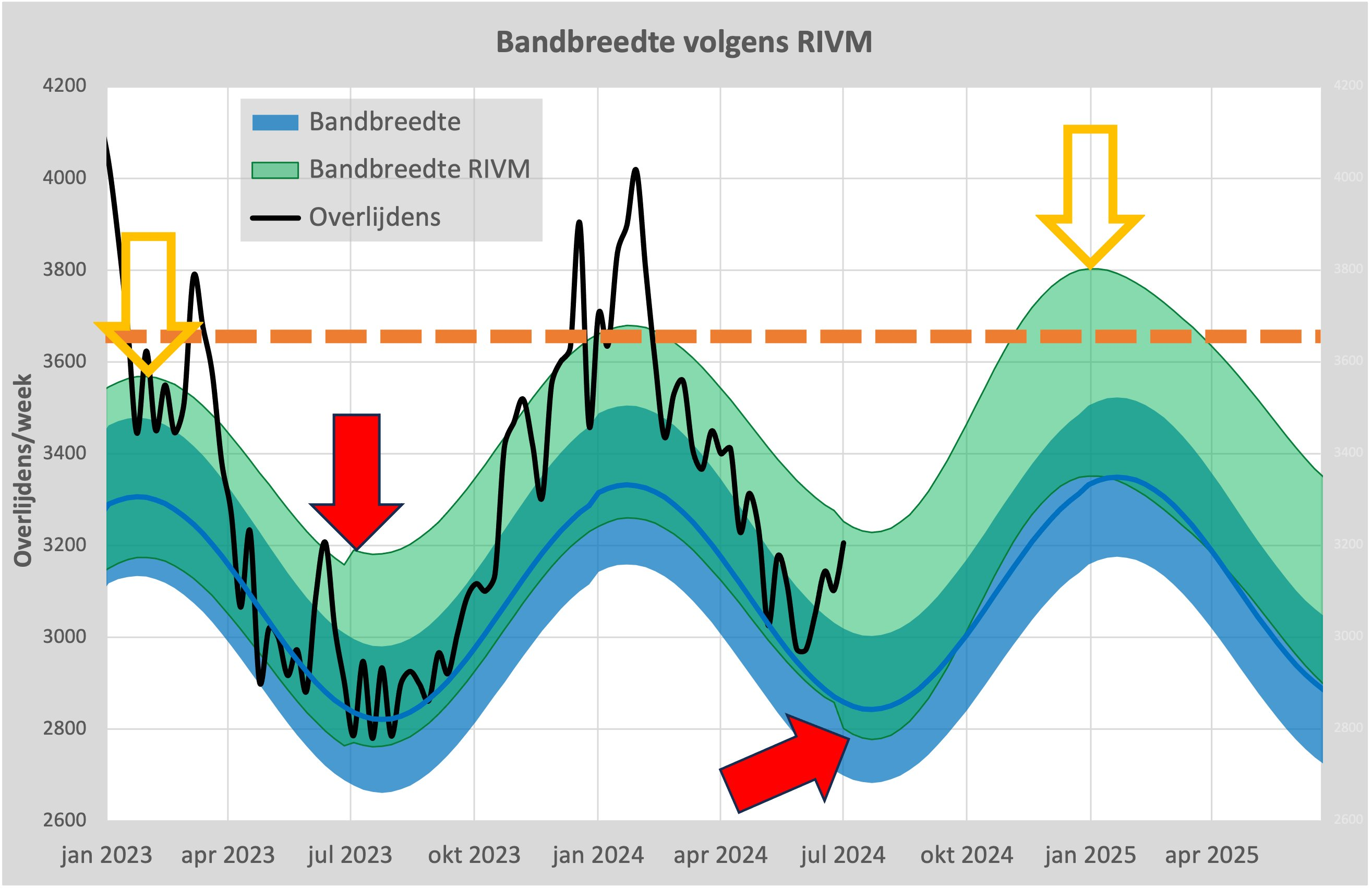
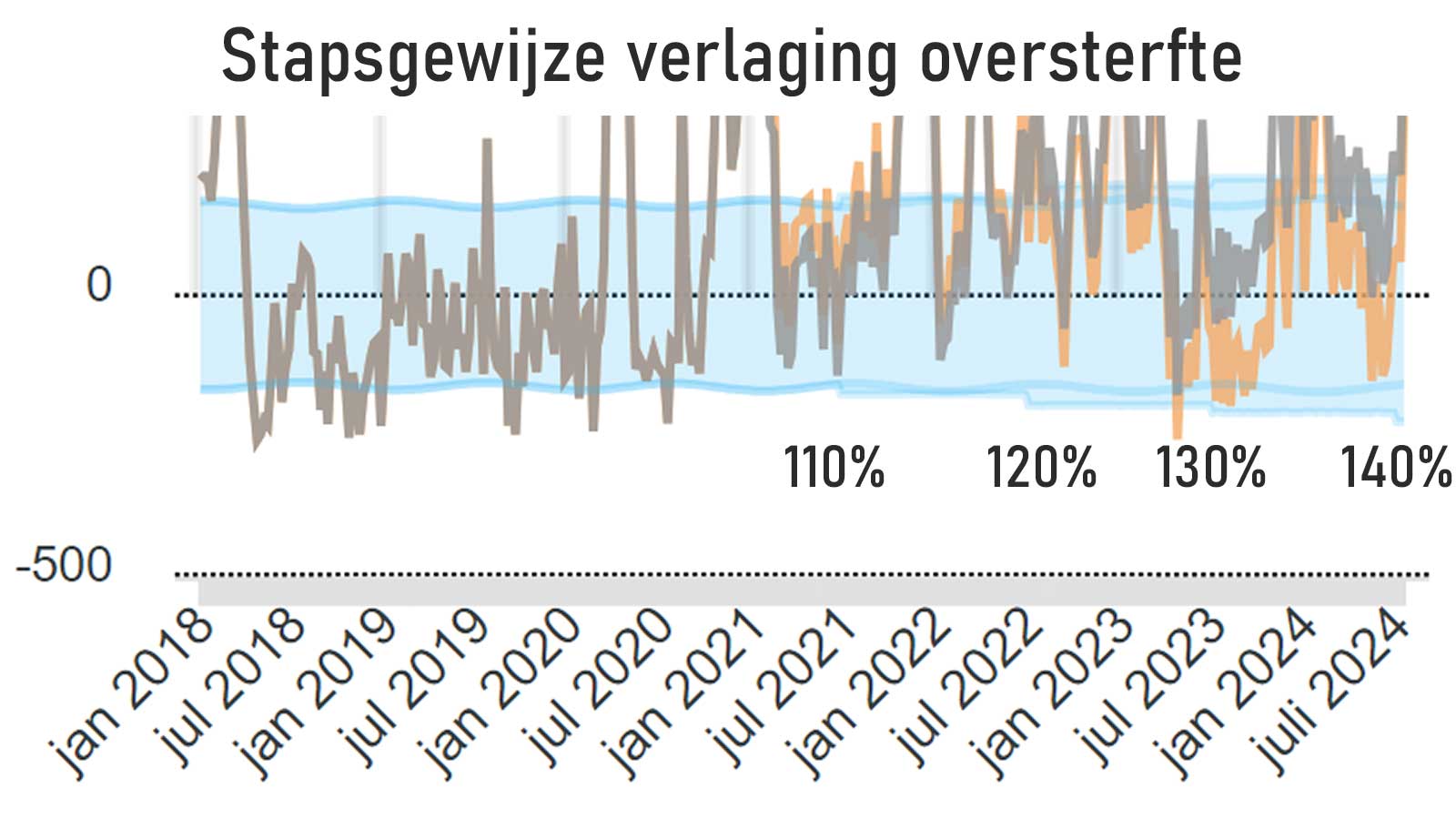
This graph shows what happens if our desired mortality level is tacitly adjusted to the average of 2021-2024 (seasonal years).
In those years, the steepest parts of each line fall earlier, which is now also reflected in the expectation of the RIVM. Those steep sections lead to more mortality as early as January than in any of the entire 2015-2019 season years.
Something irreversible took place in 2021, according to the expectations of the RIVM.
Previously, anomalies (abnormalities) in regular mortality were not included in expectations. In this way, they remained detectable.
However, RIVM has now chosen to include the anomaly in the mortality change, the trend break in 2021, in the forecast. Due to the higher expectation, considerably more deaths are needed to be able to identify excess mortality.
In recent years, the years 2015-2019 were used as the baseline, 'target mortality'. That has now been stopped. We can only guess at the reason for this change. In any case, a side effect is that there is no reason to suspect vaccines of causing serious persistent excess mortality. It disappears. After all, such a suspicion would not help with vaccination willingness.
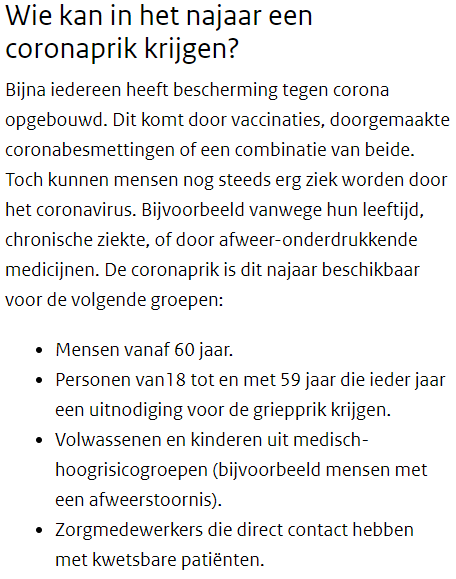
More lenient margins
Apart from that, the bandwidth has also been broadened. Compared to the standard bandwidth, the bandwidth is 40% larger than it was in 2020 as of 1 July.
As a result, the bandwidth has become considerably wider than the increase in the baseline can justify. Even if the deviations have become so much larger in the last 4 years, should that become the new norm?
This means that some extra bits of excess mortality are nibbled away. Another thing that has not been left behind.
In short: statistical choices evaporate official excess mortality.
Definition nudging
Traditionally, when average life expectancy could still be the norm for a healthy life, excess mortality was always a temporary phenomenon. In the Netherlands, this involved heat waves lasting a week or two or epidemics that lasted two to four months. It is striking that this observation is now being pushed in the direction of a definition.
In the Joint Final Report on 2020-2021 CBS and RIVM write emphatically, in a paragraph between two blank lines: "De oversterfte is het verschil tussen het waargenomen aantal overledenen en een verwacht aantal overledenen in dezelfde periode."
The Rivm describes excess mortality on its website now (July 2024) as follows: "Oversterfte is een tijdelijke, bijzondere stijging van het aantal mensen dat doodgaat in Nederland."
- Merk op dat het element "tijdelijk" is toegevoegd.
CBS has yet to finalise the further narrowed: "Oversterfte is een tijdelijke, bijzondere stijging van het aantal overledenen die samenvalt met een bijzondere gebeurtenis, zoals een griepepidemie, hittegolf of corona-epidemie."
- According to Statistics Netherlands, there is only excess mortality if it coincides with a special event. An experimental vaccination campaign seems to me to be a pretty special event. But if you don't see the causal link with that event, then the increase in mortality is not special and therefore not excess mortality?
- Correlation is causation according to CBS, but that's beside the point.
Dat "tijdelijke" moet in beide definities natuurlijk zijn "generally tijdelijke". Ze laten het tijdelijke karakter nu klinken als een noodzakelijke voorwaarde. Aanhoudende, dus niet-tijdelijke, oversterfte is dan een onmogelijkheid.
Formally, you could only speak of excess mortality when it has turned out to be temporary, i.e. it has passed. Nonsense, of course.
Die keuze voor "tijdelijk" is niet gemaakt in het belang van de volksgezondheid. Stel dat de lucht en het drinkwater door een ramp worden vervuild. Denk aan een meteoriet, een kernoorlog, wat dan ook. Ook dan zou een volksgezondheidsinstituut jarenlang in de gaten moeten houden hoe de gemiddelde sterfte afwijkt van het wenselijke sterfteniveau. Maar misschien, als de nieuwe NAVO-secretaris op de rode knop heeft gedrukt, laten we ook dan de toekomstige negatieve effecten verdampen in de gemiddeldes van de verhoogde sterftes.
Our plea is that a distinction should be made between the expected level of mortality and the desirable level of mortality. ("Gewenste sterfte" klinkt een beetje gek.) Maar ja, dan loop je wel kans dat de vaccinaties weer worden verdacht. En dat wil natuurlijk niet iedereen. In het belang van de volksgezondheid.
White Lies
The former director of the American National Institute for Public Health and the Environment (RIVM), CDC director Robert Redfield, confirms wholeheartedly that there should have been no lying about vaccine side effects in favor of vaccination readiness.
(see the video here or click on the X post)
Nederlandse media: "Ssst, dat kan ten koste gaan van de vaccinatiebereidheid!"
Corrupted data communication
They do not hesitate to provide mutilated data in WOO requests. The judge is satisfied with this openness.
The Biomedical Court of Audit had submitted a WOO request concerning vaccination dates, age category (accurate to 5 years) and date of death. At first, it turned out that the data was not there (which was demonstrably incorrect) and then suddenly they were there. The request was rejected and last week, two years after the application, it was approved in this case Court decision. The dates are online here. There are 6161 pages with 64 people per page. The State Secretary notes in the accompanying letter that it is a very large file. Indeed. It's over 1 GB of digital junk.
It starts with the fact that they are PDFs of bitmapped (moderately photocopied) pages. The quality is too poor to generate figures in an easy, automated way. See, for example, the missing minus sign in the middle line. 
Would this judge also approve of us paying our fines with a blurry photo of the appropriate amount in cash?
There was already a file circulating on social media with, as it turns out, exactly the same data (no one knew for sure). That was a modest 18 MB Excel file with readable data. Of course, the Secretary of State knew nothing about that.
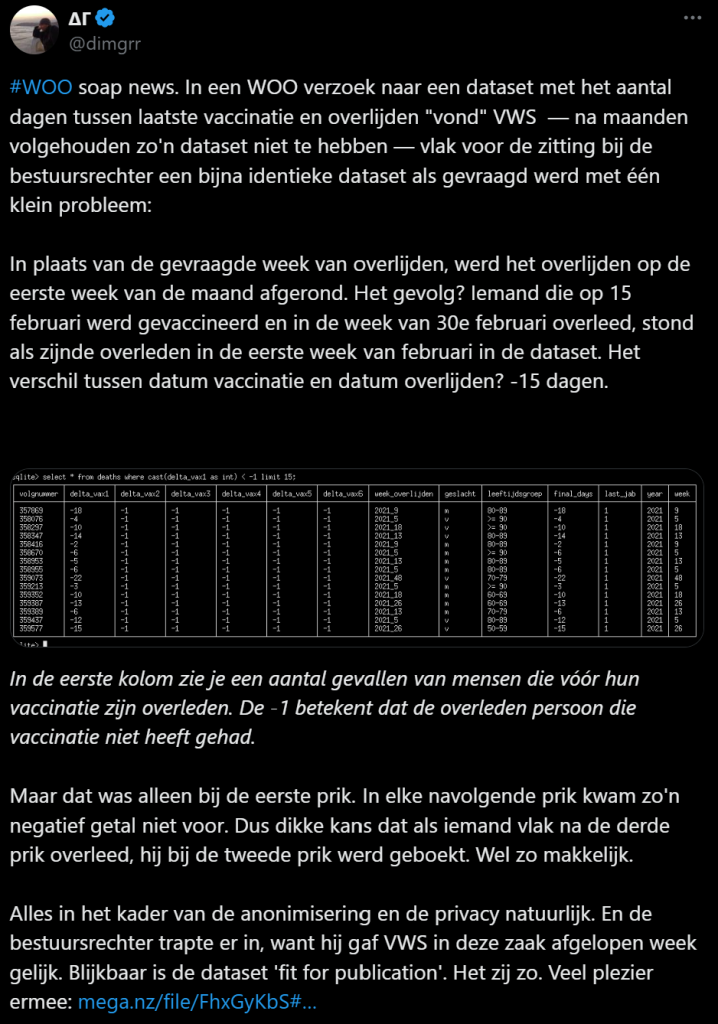
The data has been deliberately impoverished to such an extent that it has become meaningless. Someone explains it on X. Since he has blocked just about everyone I know, the screenshot is below. A judge has nevertheless found it 'suitable for publication', so the government has fulfilled the WOO obligation.
Thanks again, justice! Chapeau to the judiciary. (rule of law, anyone?)
But perhaps the judge also had in the back of his D66 mind that it actually makes no sense to discredit vaccinations again. After all, things that have been done do not take a turn and it would only harm the willingness to vaccinate. That doesn't sound very polite, but that's how you start thinking.
Hans Verwaart had in April already wrote a Substack about that data (now also a July update). In the end, he was able to make something of it on a quarterly level. After the disappearance of healthy vaccinee effects, vaccinated people continued to die more often in the course of 2022-2023 compared to the expected number.
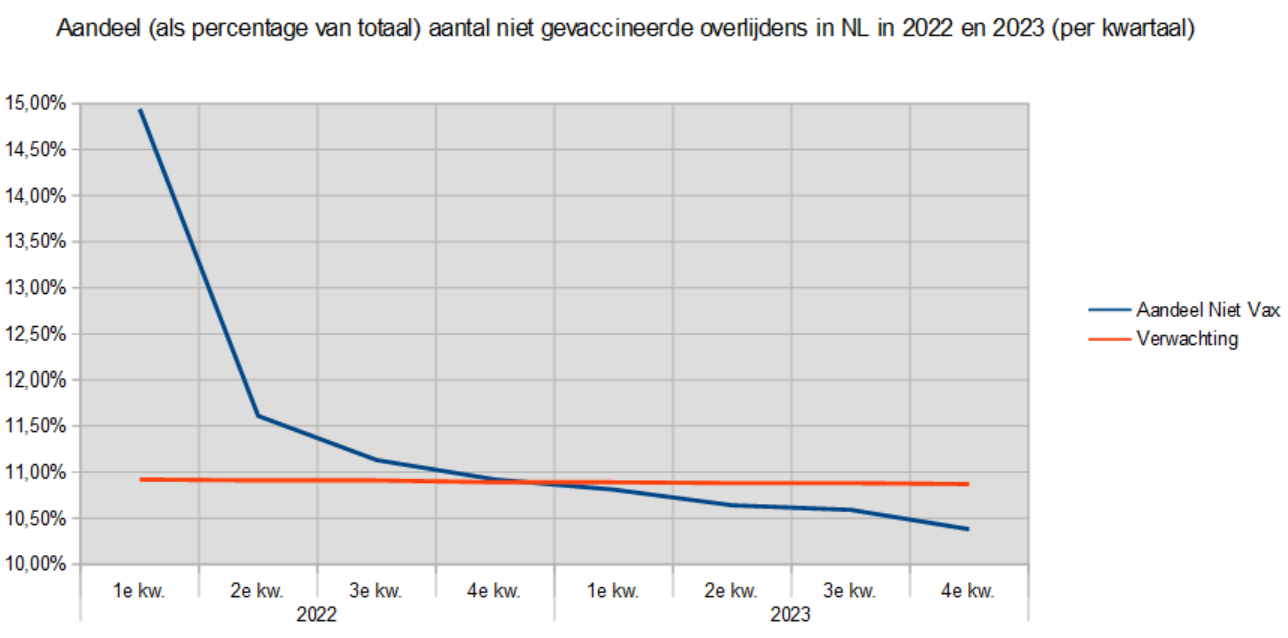
This is not encouraging for the willingness to vaccinate, but that analysis is otherwise without danger: are Substack does not go much further than a limited readership - who would no longer allow themselves to be pricked anyway.
So an Excel file has been mutilated that has also been downgraded to blurry images before publication. This is unacceptable in a democratic state governed by the rule of law. The rule of law and the media should protect us from such government stratagems. There must be a lot at stake to bring about this behaviour, not only for the ministries, institutes and experts involved, but also for the journalists and judges.
Tweaking historical figures
A pre-made expectation remains the expectation of the past, you might say. Made at the time with the knowledge of the time. Adjusting or recalculating afterwards is remarkable, especially if you tacitly replace your new calculation with the old one and pretend that you already had the prediction you made afterwards.
In a contract, you don't change a few words afterwards, even if they are only spelling mistakes. Or you can specifically mention each change.
The difference of this recalculation on total mortality is negligible, but that is not the point. Why aren't those numbers just fixed? Why is an old prediction being recalculated at all, with all the chance of unnecessary errors?
In this graph you can see the differ between the RIVM file of the last week of June 2024 and that of the First week of July 2024. Both files give the same expectation again over the same period: that of the past twelve months.
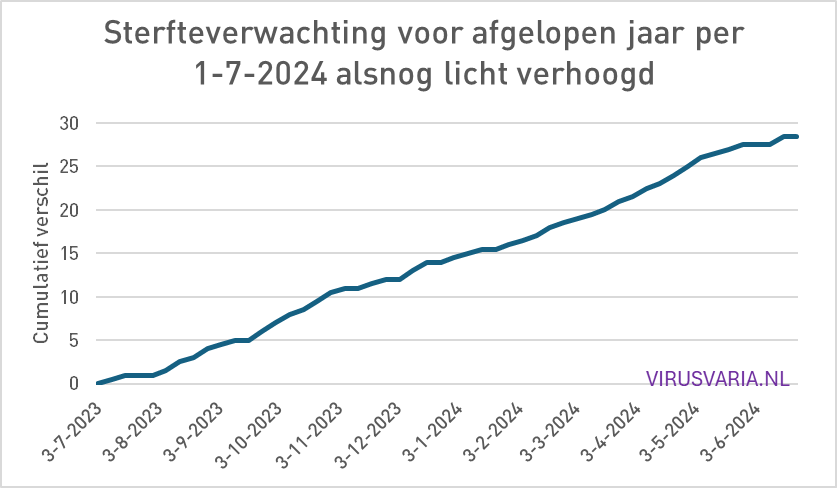
In the unnecessary recalculation, it is also striking that there are only increases, no decreases. If they are rounding differences, they all fall in the same direction.
Again: this concerns only 28 deaths in 12 months, which is of course nothing compared to the increases we had already seen. But do we still know? When Covid came knocking, every child had to be double vaccinated because otherwise it would kill grandpa and grandma (that was also made up) and the chance that a child would suffer anything from Covid was astronomically small - but it will almost certainly be your own child! That one, that's what it's all about! But those 30 people more or less in one year, well... that's a statistic.
The picture is clear
Partly due to the increasing (also medical) reports on vaccination damage and mortality (see e.g the last one by Denis Rancourt), confessions like Redfield's and all kinds of declassified documents, links are increasingly being made between the vaccinations and the unexplained excess mortality.
This is at the expense of willingness to vaccinate, while this has been central to the corona policy. Think of Hugo, the measures, the boas, the threats, the IC videos, the QR passes, videos of funeral processions, etc. etc. All culminating in Vaccinations as the Only Way Out.
The Disinformation Think Tank had the task of distorting facts or presenting them in such a way that it would benefit the willingness to vaccinate. Dissent was forcefully dismantled, banned, ignored, censored, canceled, fired. Science journalists ridiculed it.
What should happen to those people who did all that, to the then minister, to the controlling House of Representatives, etc., etc., if excess mortality remains visible and the excess mortality problem actually becomes more and more acute? Then (perhaps?) it will one day have to be recognized that the vaccinations have been an important driver of the whole misery, including that of next autumn. What should we do with all those people who are so easily fooled? Just forget and forgive? To trust...?
In the meantime, the government knows what is going on. They also understand the significance of the treason committed by the country and the people. This is evident in all the ways in which they prevent transparency: from excuses and lies to hard-nosed data fraud that manipulates, obfuscates, misplaces or otherwise does not make facts in communication available to independent researchers.
How difficult is it to provide an Excel file without amputating crucial information, such as how many days after which injection someone died - exactly the dates that were requested? And the judge thinks it's OK...
Such a judge would not have been able to assess for himself what was going on with that data. I happen to know a few judges and among them are NPO-watching NRC-reading snoops. We cannot personally blame those people for that, they had to learn very hard to achieve anything. They are products of and in a system in which the authority of government institutions is beyond dispute, especially scientific ones, such as RIVM and CBS. If judges deny that authority, they would also look at the legs under their own chair. This authority is not further substantiated and is not tested in the meantime, other than through an occasional prize festival every now and then.
The most obvious motive for these behaviors is to erase traces that lead to the recognition of one of the greatest crimes in medical history, committed against its own population.
There is little choice but for the government agencies and the media to persevere. Just as long as they insisted that Biden was sharp.
And of course: collectively continue to act as if abroad does not exist. Pretending that the vaccines are effective and safe. This includes opting for 'the new normal with more mortality' and wanting to stay far away from honest figures. This behavior works in favor of vaccination willingness and protects those who, against their better judgment, have continued to advocate for the mRNA vaccines.
But yes, even if it turns out abroad that the vaccines have caused enormous excess mortality, the Netherlands can at least point to the RIVM statistics: not with us, just look: no excess mortality, everything entirely according to expectations! And that in turn ends up in the newspaper and on TV.

Great article again, Anton. I've been following you, Maurice de Hond and Herman Steigstra since 2020. It remains frustrating that most people don't want to reflect on what has happened in recent years. Blind faith in the government and
Medics, in the meantime it has mainly become cognitive dissonance, I suspect. We will continue the fight!
Thank you Marjan! Hang in there, there's no other way.
Nicely lined up, Anton.
Have you seen the report by Rancourt et al in the meantime?
https://correlation-canada.org/covid-excess-mortality-125-countries/
What will the bunkers think of this? The cause of 'the pandemic' is the declaration of a pandemic.
It's a bit of a read:-)
I think I've seen it on X, haven't read it yet, but I have read his earlier report on the southern hemisphere. (I couldn't find the link anymore, so I've added it to the article.)
What I keep seeing is that judges rely on external expertise, such as the National Institute for Public Health and the Environment (RIVM). You can argue with that, but then you have to come up with a very good story. As far as I can see, that didn't happen in the Netherlands, possibly because legal and medical heavyweights were afraid to go against the RIVM story.
There are plenty of good stories, but the big media are propagandists. Such a story has no chance.
Agree with implausibility official story and reprehensible that people try to sweep the dangerous desire to experiment under the table.
But don't fall into easy simplifications, such as the assumption that judges have so much medical knowledge that they can recognize the mistakes of RIVM et al.
Well, then I have not made it very clear that I do not think judges are capable of doing that. In fact, this judge approves unusable junk in response to a thorough WOO request. But then again, is that incompetence or malice?
Hi Anton,
Thank you for this powerful story, you give a good overview of the state of affairs here. And maybe there is still something to do with the PDF files? Especially together with the Excel files? Really painstaking work, but it could be divided among a dozen volunteers.
Furthermore, I agree with almost everything you write here, but that of the repeat vaccination from the RIVM does not seem illogical to me – I can imagine their reasoning.
They already start with "almost everyone has built up protection" and specifically acknowledge protection from infection. Only, as far as we know (unfortunately they forgot to explain that), defenses against coronaviruses are similar to those against flu, it becomes less effective with time – even natural defenses. This is partly expressed in the sentence "Nevertheless, people can still get very sick from the coronavirus". Some people who were sufficiently immune six months ago may not be sufficiently protected next autumn.
Incidentally, my view is different from the RIVM, I try to maintain my natural immunity by staying in contact with people a lot (continuous boosting). Maybe I'm wrong, but it seems to work.
We will have to see to what extent the autumn vaccination will still be relevant in the future. So far, this is debatable, to say the least, given ACM's developments so far. A month ago, an infection was still protective, but now it is not. Still crazy.
By the way, you can't do anything with the Excel files. They were the source files for the PDFs.
Hi Anton, I tried to download the PDF files of minivws.nl, both as a subfile and also as a zip, and on two different machines. Everything failed. The zip always fails at 69 Mb. Do you happen to have the entire file?
sent by e-mail
By email? I don't see anything and how? Max. approx. 10Mb – that's 100x less than the zip file...
I've got you this link emailed, maybe ended up in the spam? I also added the link in the text above.
Thank you Anton, the link to the Excel file is good. And your answer here is only now dawning on me – so those PDFs that you can't download, on
https://open.minvws.nl/dossier/VWS-WOO/3455207-1038323-pdo
are worthless because they are just a bad copy of the mangled Excel file we already have.
Yes, indeed. Try something with it, you will see that Hans Verwaart has managed to squeeze out the most important things.
Update from Hans Verwaart
I assume that your material and interpretations/articles are kept well secured.
The government's criminalization of the spread of self-defined 'disinformation' is in full swing. Germany is leading the way in this. Usually, the Netherlands follows. The EU with Van der Leugen is also doing its utmost. See Thomas Fazi's recent article on Unherd https://unherd.com/2024/07/inside-the-eus-war-on-free-speech/
Standard security, nothing special.
Super article by the way, on Unherd!
A word about the Rancourt report. They've figured out things that I've actually been curious about for a long time. Countries compared, the measures per country, the composition of the population, geographical location, vaccination approach, etc. It has become a bulky piece of work. As a layman, I am impressed, but the debunkers will have something to say about it. According to the authors, the pattern in which 'the virus' has spread does not make any sense at all for a respiratory virus. The Netherlands is also mentioned as a country where excess mortality persists because they compare the numbers before 2020.
It is a very strange situation in which we find ourselves. Assume that other readers also occasionally feel like they're in the wrong movie. How can 'we' see so clearly what has (gone) wrong while others are convinced that there was a deadly virus circulating that was defeated by heroic virologists and sensible politicians by deploying a rapidly developed vaccine.
I recently had a few conversations with believers, and what surprised me is that they don't really know any details. Not from the severity of Covid, not from the effect of mRNA vaccines, not that there is serious excess mortality. Nor can they contradict my arguments. They have blind faith in the government and de Volkskrant. That's what their worldview is based on. They know that this gives them a limited view of the matter, but apparently they are fine with that. I tried to explain to them that I'm not just shouting something. But that my opinion is based on data. Only I don't get it from Volkskrant or NRC. The framing in those magazines is also becoming clearer and clearer to me.
If there is anyone who can explain to me why mRNA vaccines against a relatively mild respiratory virus is a good idea, I would be happy to do so and maybe I will convert. On this site, that chance is small.
Haha, no you won't find that here anytime soon. If you're on Facebook, you might want to take a look at the open group Corona Middenweg. There are some active members there, Jans Velzing and Bernard de Boeck, who might be able to convince you. I wouldn't hold my breath for it.
No, never been on facebook. Has always disliked me. From day 1. I think 'social' media is one of the biggest problems of our time. In addition to being overweight, medication use. Has to do with each other.
Without social media, you would have missed out on all the information you read on sites like this.
Of course, if mRNA were bad, the government in the UK would never help build a megafactory of Moderna, endsarc.
The good thing about mRNA is that you can develop a new vaccine very quickly and cheaply in the event of mutations. That then no longer needs to be tested and no longer validated. So cheap and fast.
There is a "small" disadvantage to it: the working principle behind mRNA vaccines appears to have disastrous side effects. That was already somewhat known but seemed to be rare; but that relative "rarity" has only really manifested itself with the massive rollout of Corona vaccines.
Here are the pros and cons of mRNA vaccines in a nutshell.
Who knows, they might be able to set a timer on it and make it cell-specific. As long as that is not possible, you can also give everyone preventive chemotherapy. Irresponsible.
Professor Theo Schetters said, with Jorn Luka on the Trueman Show, that Bourla of Pfizer had said: After corona, cancer is the next moneymaker. Count your winnings!
But don't you understand that a.o. Billie and friends their mission is fully on track to protect humanity and the earth? There are far too many people and there is far too much prosperity, our planet cannot handle that so the mission is a few billion fewer people and we can get back to work. And to prevent things from going wrong again and people multiplying like rabbits again, you need a totalitarian power that can ensure that humanity continues to get its jabs to shorten life to an acceptable standard. It has become clear that poisoning food through the food industry alone is not going to work. The people are like cockroaches, impossible to exterminate. Prosperity is also being addressed, prosperity is not good for the world at all, through an energy transition it now appears to work well, those stupid people really fall for everything. Bill wants a world full of lazy, fat, stupid, slavish, poor people. For the elite, his friends, he has a different plan, which should be twice as old as it should be and as healthy as a... yes like that actually, because nothing is really healthy anymore.
You would almost believe that there are Aliens who want to take over the world. The fact is that a lot of history also refers to this if you want to believe the videos on YouTube. But then again, what is another explanation for this super-successful mass hypnosis that has fanatically convinced many millions of people that they are doing the wrong thing, while if they were awake they would declare themselves crazy.
I don't understand why you seriously believe these kinds of stories..... Go talk to "people like that". They really don't work like that.
The correct explanation is a combination of fear, stupidity, tunnel thinking, groupthink and especially Rule of Rescue (RoR) thinking instead of utilitarian thinking. And from the pharma point of view, of course, purely selfish action. These are all very rational explanations.
Unfortunately, you come across a lot of RoR thinking: climate, migration, energy transition.
All utopian thinking to quickly "save" something here and now, but with a multitude of negative side effects. Cool analytical reasoning and drawing logical conclusions has disappeared with all those highly educated alpha and gamma educated people who have the power. In the past, power was somewhat more occupied by science-educated people and rational decisions were made by governments a little more often (but certainly not always!).
I sum up all those traits with the umbrella term "incompetence".
There are three others, financial or career motives:
– self-interest (money, position)
– bribery sensitivity
– be blackmailable
The theme of the article is interesting, but it is desirable to place the explanation of the behaviour of RIVM (and CBS) and others in a broader (international) context.
1. The average level of mortality in EU countries in the period 2016-2019 is still a good basis for determining excess mortality in 2024 and analysing the differences between EU countries. See also the recent EUROSTAT Monthly Bulletin of July 2024:
https://ec.europa.eu/eurostat/statistics-explained/index.php?oldid=509982
2.View the monthly figures of percentage changes of the countries in May 2024 compared to the average mortality in May months in 2016-2019. These are neatly spread out around 1.6% for the EU average (first line, first table and third graph). And the average level is not that high at all. So there seems to be no need to change the basis of mortality in the EU.
3.If we look further back in time (first graph and last graph), we see that in the past, excess mortality has regularly been much higher, but that a significant decline started around January 2024, which will continue until June 2024. For the first time since 2020, the EU average excess mortality has been so low for a long time (almost half a year). Is this the end of the COVID crisis in the EU?
4. Perhaps, but not for the (few) countries where the level of excess mortality is still far above 10% compared to 2016-2019. The Netherlands belongs to this group of laggards (see the third graph and the first table). This is surprising, because our neighbouring countries are not one of them. From 2021 onwards, the development of excess mortality in Belgium and Germany seemed to be linked to that in the Netherlands (Belgium was somewhat more distant). Since the end of 2023 (Belgium) and the beginning of 2024 (Germany), the Netherlands seems to have been decoupled from its neighboring countries.
N.B. This can also be seen in the last figure of the EUROSTAT monthly bulletin (press legend; then select 'Belgium', 'Germany' and 'Netherlands', perhaps turn off 'European union').
5.Why is it that the decline in excess mortality in the Netherlands is apparently being slowed down? This can only be due to specific national factors in 2020-2024. So many possible causes, including the well-known drivers of pandemic mortality, are immediately excluded. Inhibiting factors should mainly be sought at a high level: for example, the reluctance of VWS bureaucrats to switch back from a system with central control to the old, pre-pandemic, decentralized system of 'regulated market forces'. Of course, such a return means budget and job losses. This is countered with all kinds of excuses: maintaining 'pandemic preparedness', for example. It is an old and well-known problem in public finances that a 'disaster' often results in structurally higher budgets in the relevant policy areas. Such a WHO pandemic treaty is also intended, among other things, to consolidate higher budgets for health care worldwide. Rabid, of course, given the catastrophic failure of that policy (global excess mortality 20-30 million)!
6. The motive for adjusting the definition of excess mortality is now clear: RIVM and CBS are tinkering with that definition because they do not behave like public institutions but like consultants or even alibi agencies. They have to keep their clients (VWS, politicians, etc.) out of the wind by changing definitions to hide the fact that excess mortality in 2024 has changed little in the Netherlands, but it has changed elsewhere in the EU.
7. Perhaps the adjustment of the excess mortality expectation is informative after all, albeit differently than intended: the increased expectation reflects the hidden price (in human lives) of pandemic preparedness!
I only see your comment now (malfunction in the email notifications), sorry. Sounds very plausible, but a few things are not clear to me. So where do these excess mortality differences with our neighbouring countries come from? Look at Germany, where it was exactly like here.
But I don't see those excess mortality differences decoupled on OWID either... That's crazy, isn't it?
The OWD chart does not go beyond December 2023!
In my response, I talked about the fact that since the end of 2023 (Belgium) and the beginning of 2024 (Germany), the increase in mortality compared to the average in 2016-2019 in our neighboring countries has clearly decreased compared to the consistently higher level in the Netherlands.
You can read the development per country in 2023 and in the first months in 2024 from the first table of EUROSTAT. As a rule in the Netherlands, percentages above 10% are stated for all months in the half year from December 2023 to May 2024 (except for March 2024: 7.9%). For Belgium, there are only percentages in the table far below 10%, and in the last months in 2024 even only negative percentages. Germany reached the last very high rate (above 10%) in January 2024, after which there has also been a clear decline.
It may be interesting to note that, apart from the Netherlands, only islands in Europe (Ireland, Malta and Iceland) structurally exceed 10% compared to the average level of 2016-2019
will be listed in the first 5 months of 2024!
I see it, very special. Very curious to see how that continues. Eurostat also shows that we have had higher excess mortality rates than Belgium since 2021 and the difference is increasing.
In the 2-minute excess mortality debate of March 27, 2025, Thiadens (PVV) should have used the analogy with BMI as a "fixed standard" very graphically to convince his audience, the media and the public. That's just NLP.
Missed opportunity. What a bumbling.
I can have AI write an article like this:
====================
Why a fixed baseline for excess mortality is crucial
When measuring excess mortality, it is essential to use a fixed baseline rather than simply the average of recent years. This may seem like a technical detail, but it has far-reaching implications for how we identify and address public health problems.
Imagine if we adjusted the BMI standard of 25 as a healthy weight every year based on the average weight of the population. In a society where obesity is increasing, the norm would slowly but surely rise. Over time, someone who is overweight would be considered "normal" simply because the average has shifted. The real health problems would be masked by this.
Exactly the same thing happens with excess mortality if we do not use a fixed baseline. If we take the average of the previous years as the new norm every year, excess mortality gradually disappears from the picture. A persistently elevated mortality rate then becomes the new 'normal' situation, making structural problems invisible.
Take, for example, a city where the mortality rate has been 5% higher for years due to environmental pollution. With a shifting baseline, this excess mortality would no longer be noticed after a few years. The problem remains, but we have simply come to accept it as normal.
A fixed baseline works like an alarm system that alerts us when something is wrong. It enables us to recognize patterns and intervene in time for structural problems that would otherwise slowly become 'normal'.
This is also how it can be:
=========
Why a fixed yardstick is needed for excess mortality
Imagine a school where children are measured annually. The teacher uses a ruler to determine which children are growing extra. First, he neatly marks what 'normal growth' is.
But then he decides to adjust the definition of "normal growth" every year, based on how all the children have grown in the past year. What happens if the whole class starts to slow down due to a mysterious cause?
After a few years, no one notices that there is a problem anymore! Because the slowed growth has slowly become "normal" on the shifting yardstick.
This is also how it works with excess mortality. If we say every year: "the new normal is the average of recent years", then excess mortality will automatically disappear from the picture. A problem that persists becomes invisible.
It's like a scale that keeps adjusting itself. A person who gradually gains 20 kilos would never receive a warning because the scale always considers the new situation to be 'normal'.
We need a fixed yardstick – an unchanged baseline – to be able to see when something is really wrong. Otherwise, we run the risk of serious problems going unnoticed, simply because we have become accustomed to the new situation.
Misschien heeft Thiadens het ook alleen maar van horen zeggen. Ik weet niet hoe die mensen werken.