
Claim: less than 10% of deaths after vaccination are reported. As a result, the requirements set in the conditional authorisation of the Covid-19 vaccines are not met. Re-post of 4 July, moderated and supplemented with calculations.
Use of the not yet approved Pfizer-BioNTech COVID-19 vaccine, authorized for emergency use only*, is authorized under the condition that the vaccination provider is responsible for the mandatory reporting of serious adverse events, including death, regardless of attribution to vaccination.
Source: Pfizer Fact sheet *Translation dd. August 20. Later, Comirnaty was approved by the FDA in America, under the same conditions. In the Netherlands dated 13-9 still approved under conditions. For exact status per age group, click on the dangerous.
Whether an "emergency" is met is debatable because large groups are currently immunized almost symptom-free naturally. "Informed consent" is another condition that is the subject of discussion. This article is only about the obligation to report adverse reactions and in particular the obligation: reporting death after vaccination, regardless of the attribution to vaccination.
When to report and when not to report?
The rollout of vaccinations should provide information that could not emerge from the short trials, especially about side effects. In order to build up a valuable database, diseases or deaths should ALWAYS be reported within a few weeks - a commonly used period is 28 days - after vaccination, regardless of whether a relationship with the vaccination is considered likely or even possible. This is therefore a condition for the authorisation of the vaccines, a condition that is not being complied with. This can be seen in the low number of reports.
Of course, everything can be mapped out afterwards by, for example, linking deaths to vaccination databases – but by then it is far too late! That is why immediate notification is mandatory: in order to be able to intervene in time. But Lareb functions as a complaints desk with the main task: stopping difficult customers.
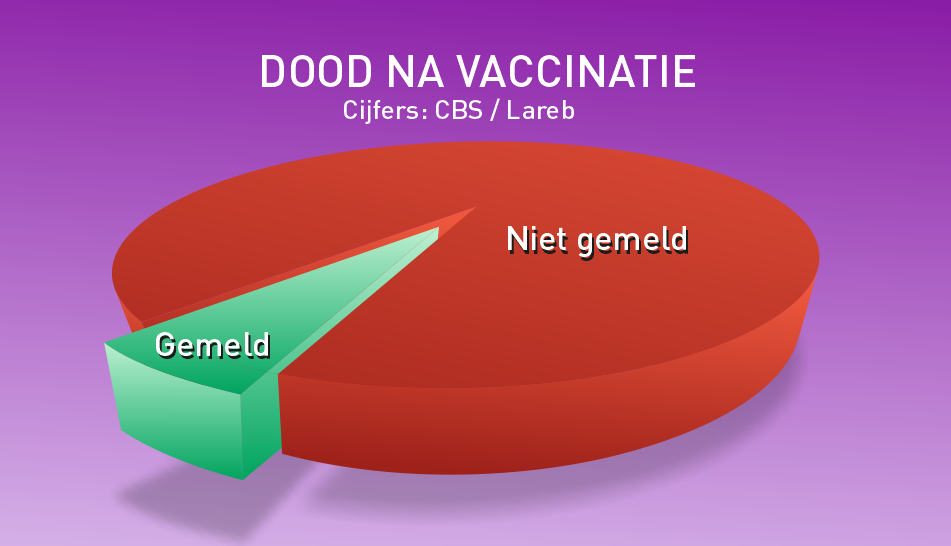
In short: If the entire elderly population of about 3.5 million people over 65 had been vaccinated and every death after vaccination had been reported, then there should have been many thousands, perhaps tens of thousands of reports of mortality to the Lareb. There are currently about 500. So even the worst possible side effect, death, is hardly reported.
To be clear: it is not about deaths on account of the vaccination. These are people who have died after they were vaccinated. Agencies such as the Lareb have the task of using the reports to find out whether there are patterns in causes of death and whether there are possible links with the vaccine. But if there are only a handful of random reports, no patterns become visible.
The numerical justification follows in the foldout below, based on data from Statistics Netherlands, the RIVM and a number of scientific articles.
Calculation: reported versus actual death after vaccination
Calculation: reported versus actual death after vaccination
Is 28 dagen wel een reële termijn om aan te houden voor mogelijke bijwerkingen? In onderzoeken naar eerdere vaccin-bijwerkingen in elk geval wel, zelfs als het om conventionele vaccins gaat. Een greep, ook van het rivm:




The numbers
More than 2,500 people over the age of 65 die every week. See Table 1; the total number minus the group of 0-65 years.
28 days is four weeks. In 28 days after vaccination, that has up to 4×2,500 = about 10,000 cases of 'death after vaccination'. guided. Remember that number:
10,000 people over the age of 65 die every month in the Netherlands.

(Calculated slightly differently: 4/52 * annual mortality in that group = expected monthly mortality. In numbers: 4/52 * 135,000 = 10,385. So that is more or less the same. You can also say that of a random group of people over 65, 0.29% die every month. That gets a bit more complicated, but do the math: that's right.)
The above assumes all people over 65. It will be objected that this is not realistic in any case because not all of them have been vaccinated. So vaccination coverage is lower, but how much lower? The most obvious thing to do is to look at the number of vaccinated people over 65 and compare it with the size of that entire age category in the population.
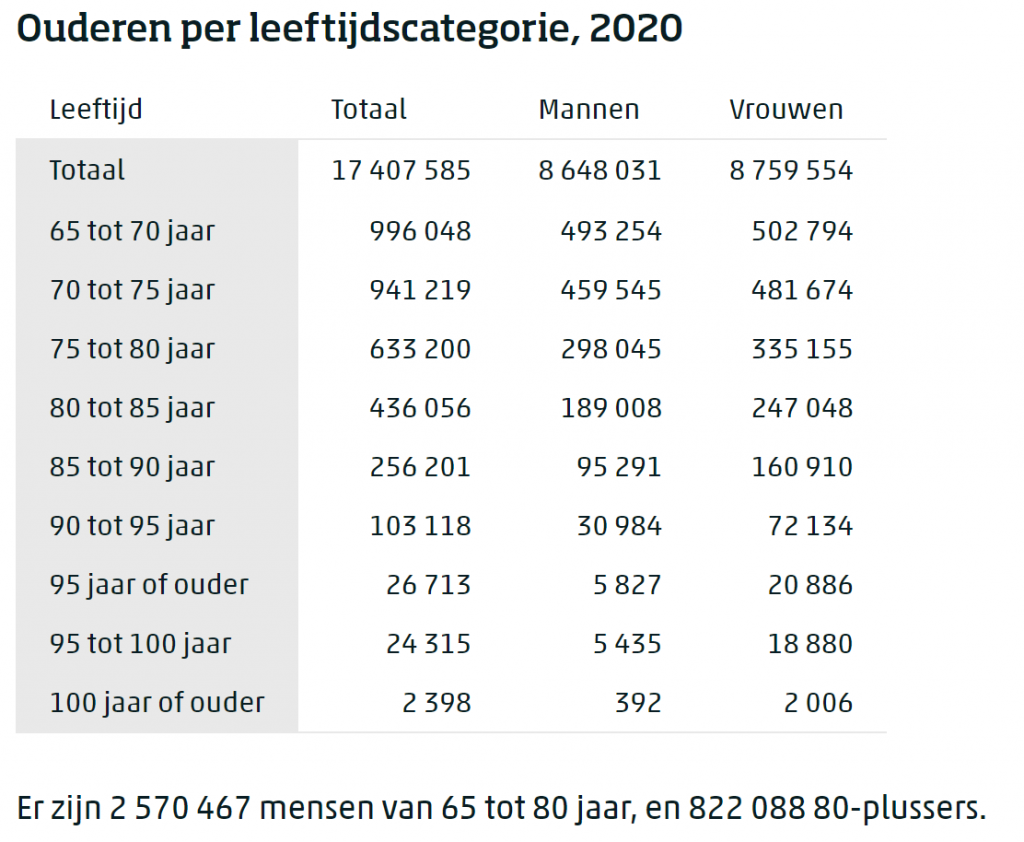
Statistics Netherlands, Table 2, shows that there are approximately 3.4 million people over 65 in the Netherlands (as of 2020). To be precise:
3,419,268 is the total number of people over 65 in the Netherlands
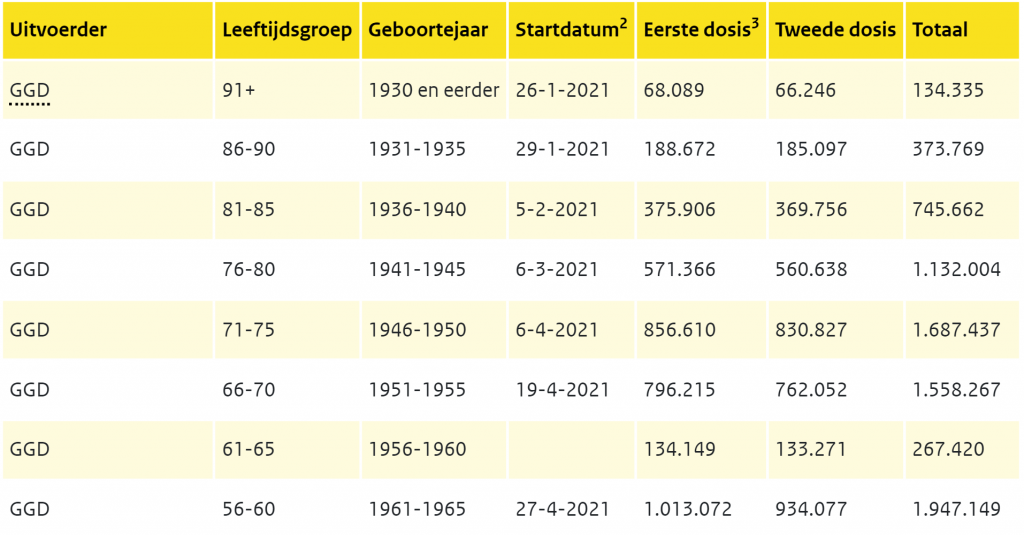
In the yellow Table 3 I added the "over-65s, second dose" together: 2.8 million. To be precise:
2,774,628 people over 65 have been vaccinated 2x
- 2,774,628 / 3,419,268 = 81% of people over 65 have been vaccinated.
- Every month, 10,000 people over the age of 65 die.
- In the first month after vaccination, you would therefore expect 8,100 reports to Lareb, if the conditions for authorisation of the vaccine were met. There are only 500 of them.
Whether you vaccinate them all on the same day or 100 per day or 100,000 per day, it doesn't matter. If you take a random group of people over 65, an average of 0.29% of them will die every month.
Statistically, 8,100 of the over-65s alone died within 28 days of being vaccinated. 461 have been reported.
Sources: Lareb, CBS [mid-August]
What have we not yet taken into account?
- Here and there some figures have been rounded down. In that period, there were actually 2,700 per week, not 2,500. This increases the number from 8,100 to 8,748 deaths after vaccination. (Now we are a bit lower: around 2,400, 2,500).
- Two injections were given per person, not one. That doubles the period for which no notification has been made. You may be heading towards 16,000. There were more first shots than second shots, the intermediate deaths have to be removed... I'm not going to recalculate that. The idea is clear.
- We only took the over-65 group because they are almost fully vaccinated. If we include the over-50s, the figures become even higher. Or you take all ages. The disadvantage of this is: the younger, the more difficult it becomes to calculate because of the gaps in vaccination coverage. Nevertheless, about 15% of total mortality is in the younger groups.
It's not even about the exact numbers but about the orders of magnitude. It is absurd to be able to calculate that 5,000, 10,000 or 15,000 people have died after vaccination, that less than 500 of them have been reported and that from those underreports it is then concluded that things are going well.
EMA itself requires, among other things, a robust risk management and safety monitoring system:
What does the reporting station report?
Lareb does not sound the alarm about this, De Jonge is silent about this. The number of reports of death at Lareb is therefore less than 10% of the statistically expected deaths after vaccination – and then I really calculate it very carefully. Are there perhaps an unusually high number of heart or brain diseases in the remaining 90%? We will only know when it is so serious that something becomes visible in the CBS or other death statistics. In any case, that is too late to intervene.
Only then may targeted research be able to show that there have been more brain/blood and heart-related deaths than normal. Is it too late for autopsies? And if deaths are not reported, what about less serious conditions?
If there are many reports from, for example, the younger age group (which is the case with some conditions), I would mainly conclude that it is more likely to be considered 'normal' in the elderly if someone gets that condition. That's all the message says. Lareb reports that it 'occurs more often in young people' while there are only 'reports' and there is no medical ground to prove it yet. This applies, for example, to thrombosis and in extremo to death. In any case, the voluntary reporting of 'suspected' side effects (i.e. "unexpected" conditions given age, for example) is at the expense of the reporting purity and is also not in accordance with the conditions of authorisation.
Many doctors and nursing homes will not like to make the link between death and vaccination. It is both extra work and it lowers the willingness to vaccinate – and it could be interpreted as a wrong act with all the liability that entails. And the side effects are so rare that it is quickly estimated that it will not be a side effect, especially in the elderly. A condition or a suspected cause of death (a GP does not do an autopsy) may not even be on the list of side effects – and you only had to report side effects, right...?
Why 'side effects'?
In Dutch we speak of: 'Mandatory reporting of serious "side effects", even if you not attributes to vaccination' – but why are they side effects? What are the side effects; If you don't attribute them to the vaccine, what do you attribute them to? Spontaneous cerebral infarctions, thrombosis, heart failure, irregularity complaints, do they fall under "side effects"? It does not give a careful impression and legally it seems to offer plenty of room for sowing doubt. In English, they have already thought about this given their "adverse events".
Perhaps one day the privacy hurdle can be overcome to link three (or two?) databases: date of death, patient file (medical history) and date of vaccination. That shouldn't be a problem anonymously and then you suddenly know a lot more. But Lareb (i.e. government) appeases unrest by saying that there are few reports. Sometimes they even say "less than expected", which in turn concludes that the vaccine in question apparently works against those specific symptoms... Data collection and analysis remains a huge sore point, but no one can do that better than the RIVM, according to the RIVM.
No control over the data
The data chaos is plaguing us from all sides. For example, Jaap van Dissel recently made it clear that the test results cannot be a guideline now because negative test results are not reported, only positive ones. So that does not give a representative picture. But isn't he in control of the data himself...? If not, then who? And don't we have a corona app for which all test results are registered? Is it impossible to add up the totals of people who tested positive and negative? And why doesn't the House ask about it? And why don't journalists put the RIVM to the test? And why is it tolerated that there is 50 lawyers are hired to find a way to refuse democratic FOI requests? It all doesn't deserve a beauty prize and, as far as I'm concerned, no medal of honour either. The uncriticalness is becoming increasingly worrying.
Possibly related articles
Only "related" if the side effects actually turn out to be related to the excess mortality because correlation is not causation: the causal relationship must be scientifically confirmed or excluded. Thorough research should show that. As long as excess mortality is not recognized and Lareb is satisfied with the reports, such an investigation will not get off the ground. After all, that would not benefit the willingness to vaccinate and neither would the pharmaceutical companies.